Peritonsillar Abscess: Symptoms, Treatment Options, and When to Go to the ER
A severe sore throat is common—but certain symptoms can signal something more serious than routine tonsillitis. A peritonsillar abscess (also called quinsy) is a throat abscess that can worsen quickly and may require urgent evaluation and treatment.
Below is an educational guide to what it is, what it can feel like day-to-day, how it’s diagnosed, how it’s treated (often with needle aspiration plus antibiotics), and the red flags that can indicate it’s time for emergency care.
What Is a Peritonsillar Abscess (Quinsy)?
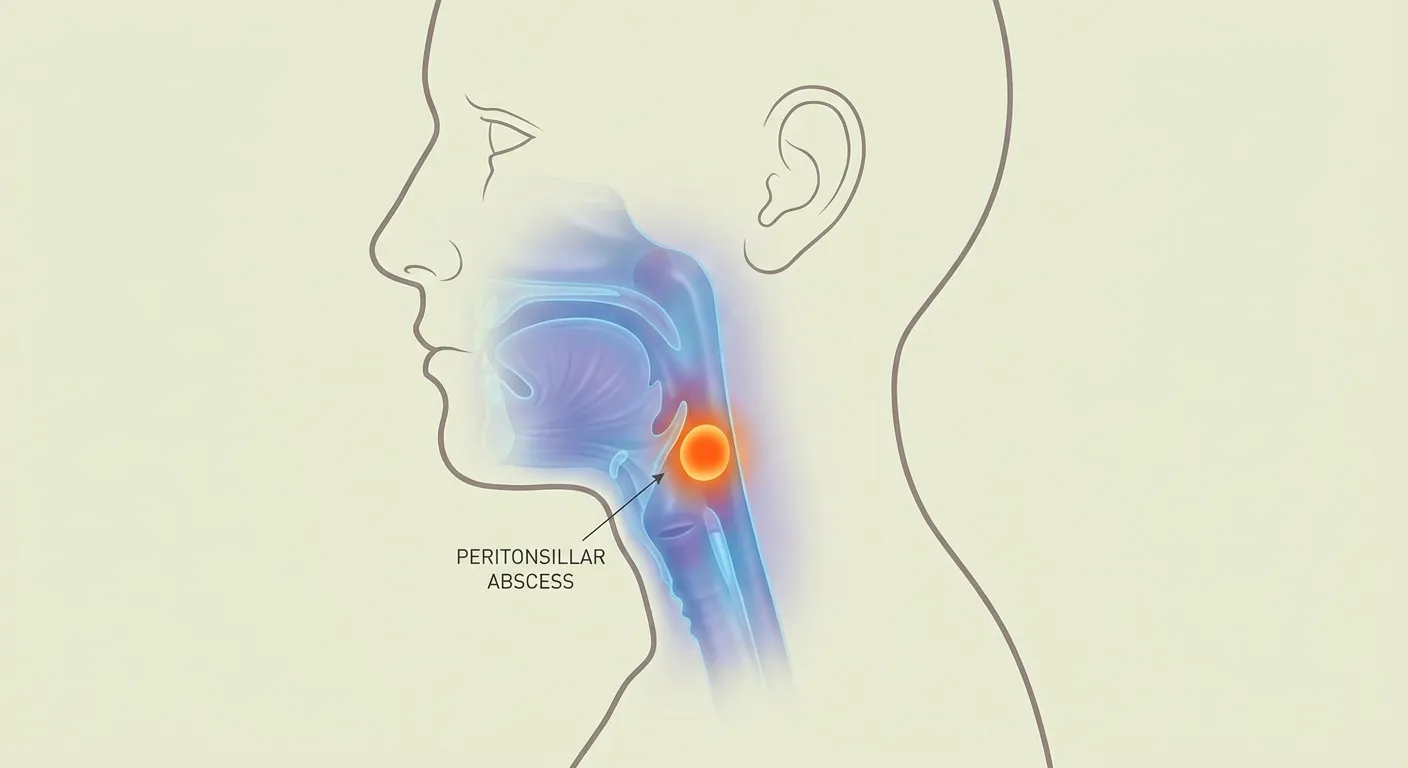
A peritonsillar abscess is a pocket of pus that forms behind or near a tonsil, usually as a complication of tonsillitis. It is one of the more common deep neck infections and can progress without prompt treatment. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
A simple way to picture it: tonsillitis is like an inflamed, infected surface, while an abscess is more like a sealed pocket of infection that the body walls off—often making it harder to treat with pills alone.
If you’d like a refresher on the underlying infection that often precedes it, see: https://sleepandsinuscenters.com/blog/what-is-tonsillitis-symptoms-causes-and-when-to-see-a-doctor
How it’s different from “regular” tonsillitis
- Tonsillitis: inflammation/infection of the tonsils.
- Abscess: a walled-off collection of pus, often more severe and frequently one-sided, which is why it’s treated differently than uncomplicated infections.
In short: a peritonsillar abscess is a walled-off infection near a tonsil that often needs drainage rather than antibiotics alone.

Peritonsillar Abscess Symptoms (What Patients Commonly Notice)
Symptoms can overlap with tonsillitis or strep throat, but a peritonsillar abscess often has a more dramatic, localized pattern. Many people describe it as a sore throat that stops feeling general and starts feeling sharply focused on one side, sometimes with escalating pain over hours to days.
Hallmark symptoms
Common peritonsillar abscess symptoms include:
- Severe sore throat (often on one side)
- Fever
- Swollen tonsil or visible asymmetry
- Trismus (difficulty opening the mouth) (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
Trismus is an especially important clue. Patients may notice they can’t open wide enough to comfortably brush teeth, yawn, or take a big bite—because the nearby muscles become irritated and tighten.
Because one-sided pain is such a key clue, see more causes of a sore throat on one side: https://sleepandsinuscenters.com/blog/sore-throat-on-one-side-causes-common-reasons-and-treatments
Other common symptoms
- A muffled “hot potato” voice
- Pain with swallowing, or trouble swallowing
- Ear pain on the same side (referred pain)
- Bad breath
- Enlarged, tender lymph nodes in the neck
A common example: someone starts with strep-like symptoms, then a day or two later they feel like swallowing glass on one side, their voice changes, and they begin avoiding food and drinks because it hurts too much.
Symptoms that can look alarming (and still need a clinician to sort out)
- The uvula appearing pushed to one side
- Noticeable swelling around the tonsil area (Cleveland Clinic, 2026: https://my.clevelandclinic.org/health/diseases/22817-peritonsillar-abscess-quinsy)
If you see obvious one-sided swelling, it doesn’t confirm an abscess by itself—but it’s a strong reason to be examined promptly.
Key idea: severe one-sided throat pain with trismus and a muffled voice should be checked by a clinician promptly.

When to Go to the ER Immediately (Red Flags)
Some symptoms suggest the throat swelling may be affecting breathing or the ability to handle secretions. These are commonly treated as emergency warning signs, because the priority is keeping the airway safe and preventing rapid worsening.
Airway and secretion danger signs
Emergency evaluation is typically recommended for:
- Trouble breathing / shortness of breath (dyspnea)
- Respiratory distress
- Drooling or inability to swallow your own saliva (not tolerating secretions) (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/; Cleveland Clinic, 2026: https://my.clevelandclinic.org/health/diseases/22817-peritonsillar-abscess-quinsy)
A practical way clinicians think about this is: if swelling or pain prevents you from swallowing normally, saliva can pool, dehydration can develop quickly, and airway risk becomes harder to predict outside a medical setting.
Other urgent reasons to seek emergency care
- Rapidly worsening throat swelling
- Inability to swallow liquids or medications (dehydration risk)
- Severe trismus (can’t open the mouth enough for exam or treatment)
- Confusion, severe weakness, or concern that infection is spreading (AAFP, 2002: https://www.aafp.org/afp/2002/0101/p93)
In plain terms, if your symptoms feel like they are accelerating rather than slowly improving, it’s safer to get evaluated urgently than to wait and see.
For help deciding the level of care, see: https://sleepandsinuscenters.com/blog/when-should-i-see-an-ent
Bottom line: breathing trouble, drooling, or inability to swallow saliva are red flags that warrant immediate ER care.
What Causes a Peritonsillar Abscess?
The most common pathway
A peritonsillar abscess often begins with tonsillitis and can progress to cellulitis and then abscess formation. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
Think of it as a spectrum: early inflammation may still be diffuse, but once pus becomes trapped in a pocket, the problem is more likely to require drainage to resolve.
Common risk factors (patient-friendly)
- Recent or recurrent tonsillitis
- Smoking
- Poor oral hygiene
- A weakened immune system (from certain conditions or medications)
Having a risk factor doesn’t mean you’ll develop an abscess—it just helps explain why some sore throats progress while others resolve without complications.
Is it contagious? The abscess itself is not contagious, though the infection that leads to it may be.
Think of peritonsillar abscess as a complication of tonsillitis that becomes a trapped pocket of infection.

How a Peritonsillar Abscess Is Diagnosed
What a clinician looks for on exam
Diagnosis often starts with the story and a focused exam. Common findings include:
- One-sided tonsil swelling
- Uvula deviation
- Muffled voice
- Trismus
Clinicians also assess hydration and safety cues—whether you can swallow sips of water, speak in full sentences, and breathe comfortably. You may be asked how quickly symptoms worsened and whether you’ve had recent tonsillitis.
Do you need imaging?
Many cases are diagnosed clinically. Imaging may be used when the diagnosis is unclear or there’s concern for deeper neck infection or complications. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
Abscess vs. not an abscess (why it matters)
This distinction changes treatment. A true abscess is a pus collection that often needs drainage, while inflammation without an abscess may be managed differently. That’s one reason evaluation is important when symptoms are severe or one-sided.
Patients sometimes say, “I’ve had bad strep before—this feels different.” That instinct can be helpful, but the exam is what determines whether there’s a drainable collection.
Diagnosis focuses on identifying whether there’s a drainable pocket of pus—because that changes treatment.

Treatment Options (What Actually Works)
Why prompt treatment is important
Treating a peritonsillar abscess promptly helps reduce pain and swallowing difficulty and lowers the risk of serious complications. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
It can also shorten the time you’re unable to eat, drink, sleep, or take medications—issues that often compound quickly when throat pain becomes severe.
Drainage is often the key step
For many patients, drainage is central to peritonsillar abscess treatment.
- Needle aspiration is a common first-line drainage approach. (University of Iowa Protocols, 2017: https://iowaprotocols.medicine.uiowa.edu/protocols/peritonsillar-abscess-pta-management; StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
In everyday terms, aspiration aims to remove the trapped pus—often relieving pressure and pain more quickly than antibiotics alone when a true abscess is present.
Other approaches that may be considered depending on the scenario include:
- Incision and drainage (I&D)
- Tonsillectomy in select scenarios (for example, recurrent severe infections) (AAFP, 2002: https://www.aafp.org/afp/2002/0101/p93)
If recurrence becomes part of the conversation, see: https://sleepandsinuscenters.com/blog/recurrent-strep-throat-vs-tonsillectomy-when-surgery-is-necessary
Antibiotics (after drainage—and sometimes before)
Antibiotics help treat the underlying infection and reduce recurrence risk. Selection varies and is based on likely bacteria, allergy history, and local resistance patterns. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
If you’ve been on antibiotics recently (or have allergies), mention that early—those details can change the safest, most effective choice.
Supportive care (symptom relief)
- Pain control (over-the-counter or prescription options as directed by a clinician)
- Hydration strategies (small sips, cold fluids, popsicles)
- Rest
A concrete tip: set a timer to sip fluids regularly. When swallowing hurts, it’s easy to fall behind on hydration without realizing it.
Outpatient vs. hospital care—how the decision is made
- Outpatient care may be possible when breathing is stable, swallowing is adequate for fluids/meds, and follow-up is reliable.
- Hospital/ER care is more likely with drooling, dehydration, significant trismus, or any airway concern. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
This decision is less about toughing it out and more about whether you can safely hydrate, take medication, and return quickly if symptoms change.
Effective treatment typically involves drainage plus antibiotics, with the care setting based on airway safety and hydration.

Recovery and At-Home Tips After Treatment
What to expect in the first 24–72 hours
After appropriate drainage and antibiotics, many people begin improving over the next few days, though throat soreness can linger. Follow-up may be recommended to ensure symptoms are resolving appropriately.
It’s also common for swallowing to improve gradually—first liquids, then soft foods, then a more typical diet as pain and swelling settle.
Practical comfort tips
- Soft foods (soups, yogurt, smoothies)
- Avoiding smoking/vaping and alcohol while healing
- Taking prescribed medications exactly as directed (including finishing antibiotics)
If you’re struggling to eat, focus on calories you can tolerate (like smoothies) and hydration first. As pain improves, nutrition is easier to rebuild.
When to call your clinician after treatment
Re-evaluation is commonly recommended if:
- Fever returns
- Symptoms worsen instead of improving
- New trouble breathing or drooling occurs (these are emergency signs)
If something feels off compared to the expected trajectory, it’s reasonable to call—especially within the first couple of days after treatment.
Most people improve within days after drainage and antibiotics; call promptly if symptoms worsen or new red flags appear.
Possible Complications (Why You Shouldn’t “Wait It Out”)
Complications clinicians worry about
- Airway compromise
- Spread into deeper neck spaces (a more severe deep neck infection) (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
These are not meant to be scary—they’re the reason clinicians take quinsy seriously and prioritize early drainage/antibiotics when appropriate.
Recurrence
Some people experience repeat episodes, particularly with recurrent tonsillitis. In those situations, tonsillectomy may be discussed as a longer-term prevention strategy on a case-by-case basis. (AAFP, 2002: https://www.aafp.org/afp/2002/0101/p93)
Serious complications are uncommon with timely care, which is why early evaluation and treatment matter.
FAQs About Peritonsillar Abscess (Quinsy)
Can a peritonsillar abscess go away on its own?
Typically, a peritonsillar abscess needs medical treatment—often drainage plus antibiotics—to reduce the risk of complications. (Cleveland Clinic, 2026: https://my.clevelandclinic.org/health/diseases/22817-peritonsillar-abscess-quinsy)
How do I know if my sore throat is just strep or an abscess?
Clues that raise concern for an abscess include one-sided severe pain, trismus, muffled voice, drooling, or worsening symptoms after tonsillitis. (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
Is needle aspiration painful?
Local numbing is typically used, and brief discomfort can occur. The exact experience varies by patient and situation.
How fast do antibiotics work?
Many people start feeling better within a couple of days after appropriate drainage and antibiotics, but when a true abscess is present, drainage (such as needle aspiration) often provides the most noticeable early relief. (University of Iowa Protocols, 2017: https://iowaprotocols.medicine.uiowa.edu/protocols/peritonsillar-abscess-pta-management)
When is a tonsillectomy recommended?
It’s often considered for recurrent severe tonsillitis or recurrent abscess, depending on individual history and risk factors. (AAFP, 2002: https://www.aafp.org/afp/2002/0101/p93)
If symptoms are one-sided, severe, or worsening, prompt evaluation helps confirm the diagnosis and guide treatment.
When to See an ENT vs. Primary Care vs. ER (Quick Guide)
Consider urgent care/primary care same day if:
- Significant throat pain + fever + swelling without breathing trouble, and swallowing is still possible
Prefer ENT evaluation when:
- Recurrent tonsillitis, recurrent abscess, or persistent one-sided symptoms (More: https://sleepandsinuscenters.com/blog/when-should-i-see-an-ent)
Go to the ER now if:
- Dyspnea, respiratory distress, drooling/inability to swallow saliva (StatPearls, 2023: https://www.ncbi.nlm.nih.gov/books/NBK519520/)
Choose the level of care based on airway safety and your ability to swallow fluids and medications.
Conclusion (Patient Takeaway)
A peritonsillar abscess (quinsy) is a serious tonsillitis complication that often requires drainage (commonly needle aspiration) plus antibiotics. Because throat swelling can become dangerous, breathing trouble or drooling are key emergency warning signs that warrant immediate evaluation. (StatPearls, 2023; Cleveland Clinic, 2026)
If you’re concerned about severe or one-sided throat symptoms, Sleep and Sinus Centers of Georgia can help guide next steps and coordinate ENT evaluation when appropriate. To get started, book an appointment at https://www.sleepandsinuscenters.com/.
If your pain is one-sided and worsening—or you have trouble swallowing saliva—seek urgent care, and go to the ER for any breathing issues.
References
- StatPearls. Peritonsillar Abscess. (Updated 2023). https://www.ncbi.nlm.nih.gov/books/NBK519520/
- Cleveland Clinic. Peritonsillar Abscess (Quinsy). (Reviewed/updated 2026). https://my.clevelandclinic.org/health/diseases/22817-peritonsillar-abscess-quinsy
- American Academy of Family Physicians (AAFP). Peritonsillar Abscess. (2002). https://www.aafp.org/afp/2002/0101/p93
- University of Iowa Protocols. Peritonsillar Abscess (PTA) Management. (2017). https://iowaprotocols.medicine.uiowa.edu/protocols/peritonsillar-abscess-pta-management
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.