Ear Infections in Children: When Ear Tubes Are the Right Answer
Ear infections are a top reason kids see the pediatrician. For many families, it feels like a loop: a cold, an ear infection, treatment as appropriate, then another episode weeks later. If that sounds familiar, you may be wondering whether ear tubes are the next step—or if waiting is better.
This guide explains what “recurrent” means, when tubes can help (and when they may not), what placement and recovery are like, newer options you may hear about, and signs fluid may be lingering and affecting hearing or speech. Clinical guidance for tympanostomy tubes is outlined by national specialty guidelines (AAO-HNS/ENT Net).
Understanding Ear Infections in Children (A Parent-Friendly Overview)
What is an ear infection (acute otitis media, AOM)? It’s an infection in the middle ear—the air-filled space behind the eardrum. Inflammation and infected fluid increase pressure, causing pain and sometimes muffled hearing. Picture a drumhead that can’t vibrate well because fluid is pushing on it.
Why children get ear infections more often: their Eustachian tubes are shorter, narrower, and more horizontal, so they clog easily; daycare and school increase viral exposure that can block drainage. Clinically, this is often a ventilation problem more than a germ problem—if the middle ear can’t drain and equalize pressure, infections and fluid are more likely to recur. Deeper explainer: https://sleepandsinuscenters.com/blog/what-is-an-ear-infection
Takeaway: Ear infections are common in kids largely because their middle ears don’t ventilate as well yet.

Symptoms Parents Should Watch For
Common signs of AOM include ear pain or ear-tugging, fever, fussiness and poor sleep, trouble hearing or not responding as usual, and sometimes ear drainage. Many parents notice night wakings that worsen when a child lies flat because pressure shifts.
Clues that fluid may be lingering after infection: muffled hearing or rising TV volume, speech delay or unclear speech, not hearing soft sounds, occasional balance issues, and a “full” sensation (older kids). A frequent parent observation—“He doesn’t seem to hear me unless I’m right next to him”—often prompts hearing checks and a look for persistent fluid.
Takeaway: If hearing, speech, or balance seem off, lingering middle-ear fluid may be the reason.

Causes and Risk Factors (Why It Keeps Coming Back)
The Eustachian tube is the middle ear’s ventilation and drainage pathway. When it doesn’t open well—often from swelling due to colds or allergies—fluid gets trapped. Trapped fluid can become infected (AOM) or persist without infection but still affect hearing (otitis media with effusion, OME). Think of the tube as the room’s vent and drain; if it’s blocked, the room stays damp and problems recur.
Common risk factors include frequent colds from daycare or school, chronic nasal congestion or allergies in some kids, secondhand smoke exposure, and family history. These patterns are well described in clinical overviews.
Takeaway: Recurrence often reflects a ventilation issue plus common exposures—not parenting missteps.
When Do Ear Infections Become “Recurrent”?
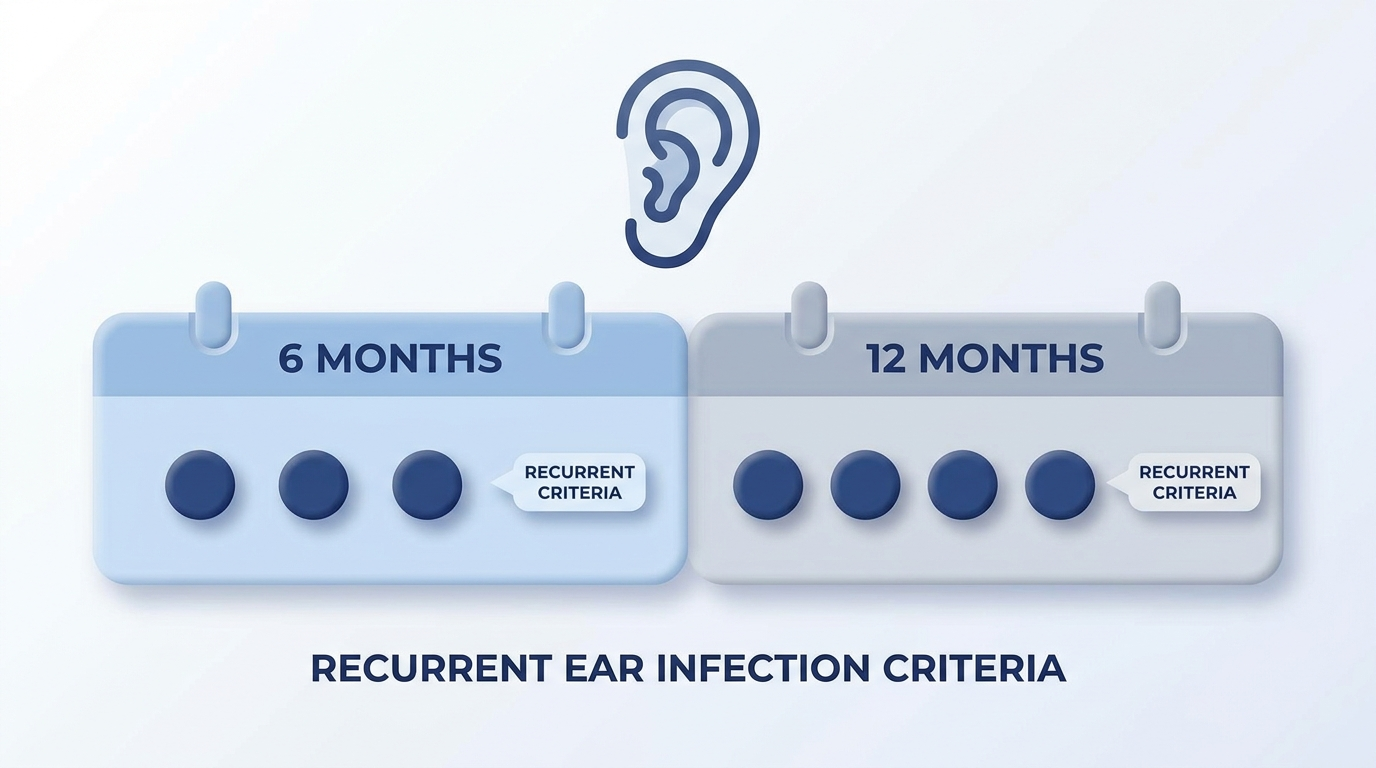
Clinicians commonly define recurrent AOM as 3 or more infections in 6 months, or 4 or more in 12 months. Counts help, but what matters greatly at evaluation is whether fluid is present and how much the episodes affect life (sleep, missed daycare/school, repeated antibiotics).
What counts as a separate infection? Generally, symptoms improve or resolve and then return later with a new exam confirming infection. Keeping a simple log of dates, which ear, treatments, and follow-up fluid status makes ENT visits faster and clearer.
Takeaway: Counting episodes guides decisions, but the ear exam—especially fluid—drives next steps.
When Ear Tubes Are the Right Answer (Decision-Making Criteria)
Ear tubes (tympanostomy tubes) are tiny cylinders placed through the eardrum to let air in and help fluid drain. They may be discussed for frequent, recurrent AOM when fluid is documented and the overall burden is high; for chronic fluid (about 3 months or more) linked to hearing loss, speech or developmental concerns, or quality-of-life issues; or when symptoms persist or keep returning despite appropriate treatment. More on lingering fluid and hearing: https://sleepandsinuscenters.com/blog/chronic-ear-fluid-and-hearing-loss-causes-symptoms-treatment
Takeaway: Tubes are considered when recurrence and/or persistent fluid are documented—especially when hearing, development, or family life are affected.
What Ear Tube Placement Is Like (Procedure and Recovery)
Traditional tube placement involves a tiny opening in the eardrum (myringotomy) and placing the tube through that opening. In children, it’s typically done with general anesthesia for comfort and stillness. The procedure is brief, with no external incisions—everything is done through the ear canal.
Recovery is usually quick: same-day discharge, mild and short-lived discomfort for many children, and routine follow-ups to check tube position and ear health. Tubes often come out on their own over time, though timing varies. Our team focuses on clear expectations around aftercare, follow-ups, symptom tracking, and hearing concerns.
Takeaway: Placement is brief, recovery is generally quick, and follow-up keeps ears and hearing on track.
Newer Options and Emerging Alternatives Parents May Hear About
In-office ear tube placement (for select patients) may be possible with systems like Hummingbird TTS, potentially avoiding general anesthesia. Suitability depends on age, anatomy, comfort with an in-office approach, and clinician recommendation.
Over-the-counter products marketed for ear symptom relief (for example, ClearPop) are not replacements for medical evaluation or established treatment; evidence may be limited, so discuss with your child’s clinician.
Takeaway: Newer tools exist for select situations, but choices should be guided by your clinician and current evidence.
Treatments Before Tubes (and Why They Sometimes Aren’t Enough)
Not every ear infection needs immediate antibiotics. Depending on age, symptoms, and the exam, watchful waiting or targeted antibiotics may be recommended. If watchful waiting is suggested, it means careful monitoring with clear guidance on pain control and when to escalate.
Plans may also address contributing factors when relevant: easing chronic nasal congestion or allergy symptoms, reducing secondhand smoke exposure, and staying current on vaccines and hand hygiene to reduce respiratory infections. These steps help lower risk but may not fully prevent recurrence.
Takeaway: Many children improve with time and targeted care—tubes are for when problems persist or keep returning.
Lifestyle Tips for Families Dealing With Frequent Ear Infections
Comfort measures during infections: prioritize rest and fluids, use fever and pain reducers only as directed by your clinician, and avoid putting objects (including cotton swabs) into the ear canal. If there is ear drainage, gently wipe the outer ear rather than inserting anything into the canal.
Prevention habits: maintain a smoke-free environment and reinforce handwashing and illness-limiting habits during peak cold seasons.
Takeaway: Simple comfort and prevention steps help, but persistent symptoms should be checked by a clinician.
When to Call the Doctor (and When It’s Urgent)
Call your pediatrician or ENT if symptoms last more than 48–72 hours, worsen, or keep returning; if there are high fevers, significant ear pain, or new ear drainage; or if you notice hearing concerns, speech delay, or reduced responsiveness to sound.
Seek urgent or emergency care for stiff neck, severe headache, swelling behind the ear, marked lethargy, signs of dehydration (especially in infants and toddlers), or severe ear pain with significant redness or swelling around the ear. This guidance is for safety awareness, not diagnosis.
Takeaway: Persistent, worsening, or concerning symptoms deserve timely medical attention.
FAQs About Ear Tubes in Children
How do I know if my child needs ear tubes? Clinicians may consider tubes for recurrent infections, especially when fluid is present at evaluation, or for persistent fluid lasting about 3 months or more with hearing, speech, developmental, or quality-of-life concerns.
Do ear tubes stop all ear infections? Not always. Many children have fewer infections, and when infections occur, fluid may drain more easily through the tube, but infections can still happen.
Are ear tubes safe? They are commonly used and generally safe. Potential risks include drainage, blockage, or (less commonly) a persistent eardrum opening after the tube comes out; your clinician will review these in context.
Can ear tubes help hearing? Often yes, when hearing problems are due to persistent middle-ear fluid. Hearing testing may be recommended.
What about water exposure (baths, pools)? Guidance depends on the child, water type, and symptoms. Details: https://sleepandsinuscenters.com/blog/ear-tubes-and-water-safety-for-kids-essential-rules-parents-must-know
Takeaway: Ear tube decisions are individualized and made with your child’s clinician.
Conclusion: A Clear Next Step for Parents
When infections keep cycling, the key question is “Why does this keep happening?” Ear tubes are often considered when infections meet recurrence criteria and/or chronic fluid is affecting hearing, comfort, sleep, or development. If you have concerns about recurrent infections, hearing, speech, or persistent fluid, talk with your pediatrician or an ENT specialist. To consult an ENT at Sleep and Sinus Centers of Georgia: https://sleepandsinuscenters.com/appointments
Takeaway: If ear infections keep cycling or hearing seems affected, ask whether tubes or other options make sense.
Medical disclaimer: This article is for general education only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Sources
National Library of Medicine (PMC, 2022): https://pmc.ncbi.nlm.nih.gov/articles/PMC9097734/
AAO-HNS Tympanostomy Tubes Guideline (ENT Net): https://www.entnet.org/quality-practice/quality-products/clinical-practice-guidelines/tympanostomy-tubes-in-children/
CHOP (2023): https://www.chop.edu/news/health-tip/3-signs-your-child-may-need-ear-tubes
UVA Health (Ear Tubes): https://childrens.uvahealth.com/treatments/ear-tubes
Preceptis Medical—Hummingbird TTS: http://preceptismedical.com/
ClearPop About: http://clearpop.com/about/
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.