
Best Antihistamine for Clogged Ears? Options for Allergy‑Related Ear Fullness and When to Get Help
That “plugged,” “full,” or “underwater” ear feeling can be frustrating—especially when it comes and goes with allergy season. One possible cause is Eustachian tube dysfunction (ETD), which can happen when allergy‑related swelling and mucus interfere with how the ear equalizes pressure. The Cleveland Clinic notes that ETD can lead to ear fullness, popping, and muffled hearing, and it’s often linked to inflammation from conditions such as allergies.¹
This guide explains over‑the‑counter options people often consider when allergies contribute to ear pressure, how antihistamines compare with decongestants, and what else may support relief (like nasal steroid sprays and saline). You’ll also learn when persistent symptoms deserve evaluation—because “clogged ears” can mean different things depending on the cause.
For a deeper background, see our related guide on Eustachian tube dysfunction (ETD): https://sleepandsinuscenters.com/blog/eustachian-tube-dysfunction-symptoms-causes-effective-treatment-options

What Does “Clogged Ears” Feel Like?
People describe allergy‑related ear congestion in a few classic ways:
– Ear fullness/pressure, like being on a plane
– Muffled hearing, as if sound is “underwater”
– Popping/clicking with swallowing or yawning
– Mild ear discomfort
– A sense that the ear “won’t open”
These align with typical ETD symptoms described by the Cleveland Clinic.¹ In simple terms, the Eustachian tube helps balance pressure; when it doesn’t open smoothly, you can feel pressure and hear popping even without sharp pain.
If you want more background on ear congestion causes and at‑home strategies, you can also read: https://sleepandsinuscenters.com/blog/ear-congestion-causes-and-relief-effective-tips-to-clear-blocked-ears
When symptoms may NOT be allergies
Not every clogged‑ear sensation is from allergies or ETD. A prompt evaluation is especially important for symptoms such as:
– Sudden hearing loss
– Severe pain
– Ear drainage, bleeding, or fever
– Significant dizziness/vertigo
– New or worsening symptoms on one side
These can overlap with other ear conditions that need timely care.¹ If you’re unsure, it’s reasonable to treat “new and severe” symptoms differently from familiar, seasonal symptoms you’ve had before.
In short: familiar, seasonal ear fullness may relate to allergies and ETD, but red‑flag symptoms should be evaluated promptly.
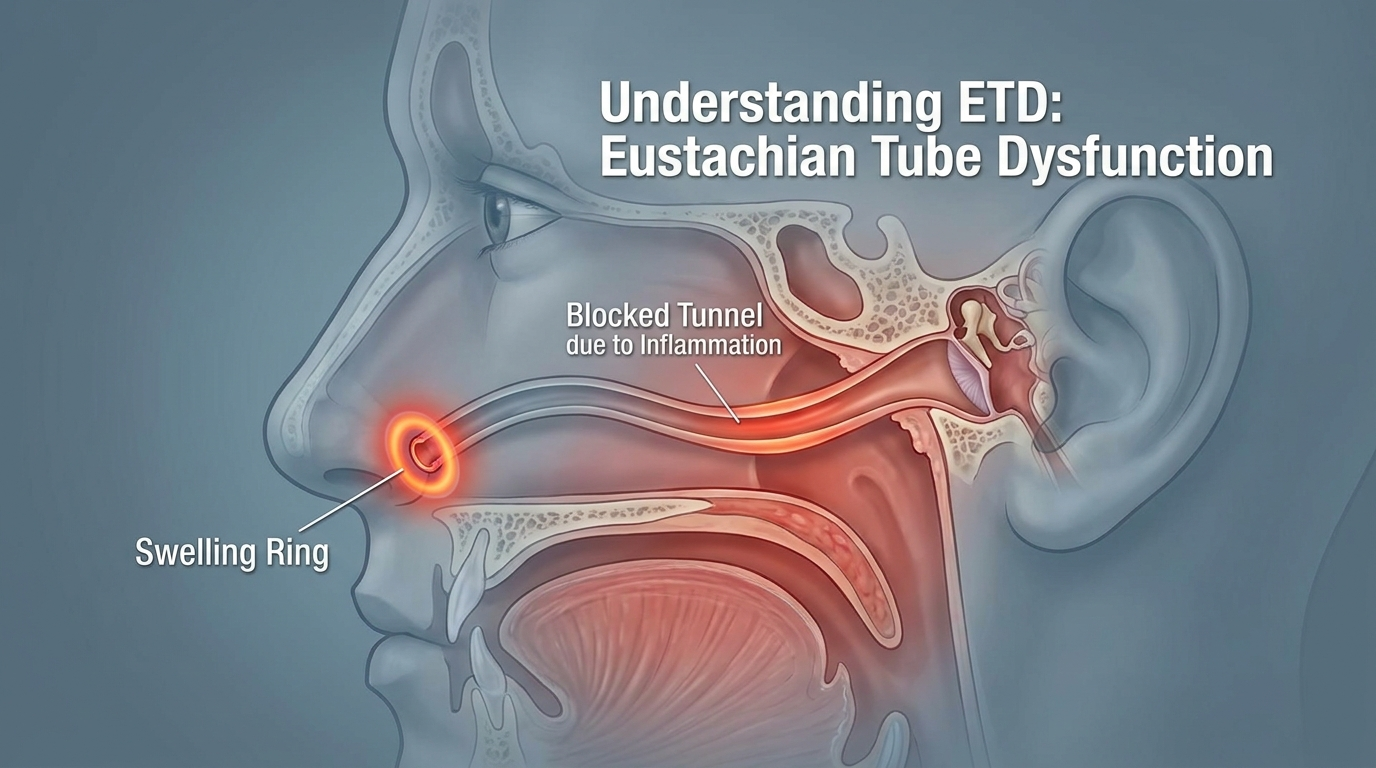
Why Allergies Can Cause Clogged Ears (The ETD Connection)
The Eustachian tube in plain language:
– Equalize pressure on both sides of the eardrum
– Drain fluid from the middle ear
How allergies can trigger ear pressure
Allergies can set off inflammation in the nose and upper airway. Swelling near the Eustachian tube opening can make it harder to ventilate and drain properly. The result may be pressure, popping, and muffled hearing—classic ETD‑type symptoms.¹ Medical literature also discusses the relationship between inflammatory conditions (including allergic processes) and ETD.² Even without obvious nasal stuffiness, “hidden” swelling can still disrupt pressure regulation.
Bottom line: allergy‑driven swelling near the Eustachian tube can contribute to ear fullness, popping, and muffled hearing.

Antihistamines That May Help When Allergies Contribute to Ear Fullness (Top OTC Picks)
When allergies are part of the picture, an antihistamine may help control allergy symptoms that can contribute to nasal swelling and ear pressure. Many people comparing options start with “second‑generation” antihistamines because they usually cause less drowsiness than older options. Individual response varies.
Important note: Dosing, interactions, and suitability differ by product and person. Always follow labels and consider asking a pharmacist or clinician which option fits your health history.
Why second‑generation antihistamines are often considered
– Commonly used for seasonal and year‑round allergies
– Usually cause less drowsiness than first‑generation antihistamines
– Practical for daytime use and ongoing allergy management³
Common OTC options
– Cetirizine (Zyrtec): Often chosen when symptoms feel more intense; may cause mild drowsiness in some (follow label directions)
– Loratadine (Claritin): Often preferred when minimal sedation is a priority; some find it milder
– Fexofenadine (Allegra): Very low rate of drowsiness for many; certain fruit juices can affect absorption
How to choose among them
– If drowsiness is a concern: loratadine or fexofenadine are commonly considered
– If overall allergy symptoms are stronger: cetirizine may be worth a try
– Track what you take and how symptoms change for a week or two
In short: second‑generation antihistamines are commonly used for allergy control with less drowsiness, but the “best” choice depends on your symptoms and tolerance.

Antihistamines vs. Decongestants: Which Helps Ear Pressure Faster?
What antihistamines do
Antihistamines help with allergy symptoms. For ETD related to allergies, consistent use may support improved comfort over time, but they do not reliably provide immediate “ear popping” relief for everyone.
What decongestants do
Decongestants may temporarily reduce nasal swelling and help some people feel more pressure relief, but they are not appropriate for everyone. Options include:
– Pseudoephedrine (behind the counter in the U.S.): May help with pressure and congestion; can raise blood pressure/heart rate and cause jitteriness or insomnia; interacts with certain medications
– Phenylephrine (oral): Widely available OTC, but evidence for effectiveness at standard oral doses is limited; in 2023 a U.S. FDA advisory committee concluded current oral doses were not effective for nasal congestion
– Topical nasal decongestant sprays (e.g., oxymetazoline): Can provide short‑term relief but should not be used for more than 3 days to avoid rebound congestion
Combination products (antihistamine + decongestant)
Some products include both when allergy symptoms and significant congestion occur together. Suitability depends on your health conditions and medications; ask a pharmacist or clinician before using, especially if you have high blood pressure, heart disease, thyroid disease, glaucoma, enlarged prostate, are pregnant or breastfeeding, or take other stimulants/MAOIs.
For a deeper comparison of roles and timing, see: https://sleepandsinuscenters.com/blog/decongestant-vs-antihistamine-when-to-use-each-for-allergy-relief
Key point: decongestants can feel more “unclogging” for some in the short term, while antihistamines target allergy symptoms; safety and suitability should guide the choice.
What About Benadryl (Diphenhydramine) and Other First‑Generation Antihistamines?
When they might be used
First‑generation antihistamines (like diphenhydramine/Benadryl) are sometimes used short‑term, especially at night, when allergy symptoms interfere with sleep.
Why they’re usually not first‑line for daytime ETD symptoms
These older antihistamines commonly cause more sedation and next‑day grogginess and can increase dry mouth. For routine daytime allergy management, second‑generation options are usually preferred because they tend to cause less drowsiness.³ Extra caution is needed for children, older adults, and anyone sensitive to sedation.
Takeaway: first‑generation antihistamines may help at night but are typically not ideal for daytime, ongoing ETD‑type symptoms due to sedation.

Other Treatments That Often Help Alongside Antihistamines
Nasal steroid sprays (for underlying nasal inflammation)
Nasal steroid sprays (e.g., fluticasone, triamcinolone, budesonide) target nasal inflammation near the Eustachian tube opening. They work best with consistent daily use and proper technique; effects are gradual rather than instant.
Saline rinses/sprays
Saline can help rinse away allergens and thin/clear mucus. If you use a rinse (not just a spray), use sterile or distilled water (or previously boiled and cooled water).
Pressure‑equalizing maneuvers (gentle only)
– Swallowing, yawning, chewing gum
– A very gentle Valsalva maneuver (avoid forceful blowing)
In brief: pairing allergy control with nasal steroid sprays, saline, and gentle pressure‑equalizing maneuvers can support comfort over time.
Lifestyle Tips to Help Prevent Allergy‑Related Ear Clogging
Reduce exposure when counts are high
– Keep windows closed on high‑pollen days
– Shower and change clothes after time outdoors
– Consider HEPA filtration in key rooms if helpful
Hydration and humidity basics
– Stay hydrated to help keep mucus thinner
– Aim for balanced indoor humidity to reduce irritation
Travel/altitude tips
– If you’re prone to ETD, stay on top of allergy control during travel seasons
– Avoid flying with significant cold/sinus symptoms when possible
Short version: lowering allergen exposure and managing indoor air and hydration can make ear‑pressure flares less frequent and intense.
When to See a Doctor
Seek urgent care right away if you have:
– Sudden hearing loss
– Severe ear pain
– Ear drainage or blood
– Significant dizziness/vertigo
– Facial weakness or severe headache
Schedule a visit with an ear, nose, and throat (ENT) specialist if:
– Ear pressure lasts more than 1–2 weeks despite OTC measures
– Symptoms recur with allergy seasons
– You suspect chronic ETD or middle ear fluid
– Symptoms are one‑sided or progressively worsening
The Cleveland Clinic notes that persistent ETD‑type symptoms should be evaluated to confirm the cause and rule out other problems.¹
Essential point: if symptoms are severe, one‑sided, or persistent despite OTC care, an in‑person evaluation is the safest next step.
FAQs
Q: What is the “best” antihistamine for clogged ears from allergies?
A: There isn’t a single best option for everyone. Many people start with second‑generation antihistamines such as cetirizine, loratadine, or fexofenadine because they generally cause less drowsiness than older options and may help with allergy symptoms. Individual response varies.¹ ³
Q: How long does it take for an antihistamine to help ear pressure?
A: Some allergy symptoms can improve within hours, but ETD‑related ear pressure may take longer, especially if inflammation and mucus are significant. Consistent use during ongoing exposure (like pollen season) often matters more than taking it only on the worst days.
Q: Is a decongestant better than an antihistamine for unclogging ears?
A: Decongestants may reduce nasal swelling more quickly for some people and feel more “unclogging” in the short term. Antihistamines help manage allergy symptoms. Not everyone can safely take decongestants, and oral phenylephrine has limited evidence of benefit. Ask a pharmacist or clinician which approach fits your situation.
Q: Can allergies cause fluid in the ear?
A: Allergies can contribute to ETD, and ETD can make it harder for the middle ear to ventilate and drain properly—sometimes leading to trapped fluid/pressure. Persistent fluid should be evaluated.¹
Q: Why do my ears clog even when my nose isn’t very congested?
A: Even if you don’t feel very “stuffy,” the area around the Eustachian tube opening can still be inflamed. That swelling alone can trigger pressure and muffled hearing.
Conclusion: Key Takeaways and Next Steps
– If your symptoms suggest allergy‑related ear fullness, a second‑generation OTC antihistamine (cetirizine, loratadine, or fexofenadine) is a reasonable place to start, recognizing that response varies.
– If pressure feels intense, a decongestant may offer quicker relief for some—but it isn’t appropriate for everyone, and oral phenylephrine has limited evidence of benefit. Confirm safety with a clinician or pharmacist.
– For recurring or persistent symptoms, identify triggers and consider a more targeted plan, including nasal steroid sprays and saline rinses used consistently.
If symptoms keep returning each season, Sleep and Sinus Centers of Georgia offers allergy testing to help pinpoint triggers: https://sleepandsinuscenters.com/allergy-testing
You can also book an appointment to discuss recurring ear pressure, ETD concerns, and next‑step options: https://www.sleepandsinuscenters.com/
In summary: combine allergy management with safe decongestant use (when appropriate), nasal care, and timely evaluation to address ear fullness more effectively.
Sources
1. Cleveland Clinic — Eustachian Tube Dysfunction: https://my.clevelandclinic.org/health/diseases/22527-eustachian-tube-dysfunction
2. NIH/PMC — ETD and inflammation discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC7170417/
3. Overview of second‑ vs first‑generation antihistamines and sedation differences (general reference): https://www.boltpharmacy.co.uk/guide/best-allergy-medication-for-clogged-ears
4. FDA Advisory Committee (2023) — Oral phenylephrine effectiveness discussion: https://www.fda.gov/advisory-committees/advisory-committee-calendar/september-11-12-2023-nonprescription-drugs-advisory-committee-meeting-announcement-09112023-09122023
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.





