Acute Rhinosinusitis: Symptoms, Causes, and Treatment Options
Congestion, facial pressure, and thick drainage can make anyone say, “I think I have a sinus infection.” But in many cases, the problem is acute rhinosinusitis—a short-term inflammation of the nose and sinus passages that often improves with time and supportive care rather than antibiotics, especially when the cause is viral.
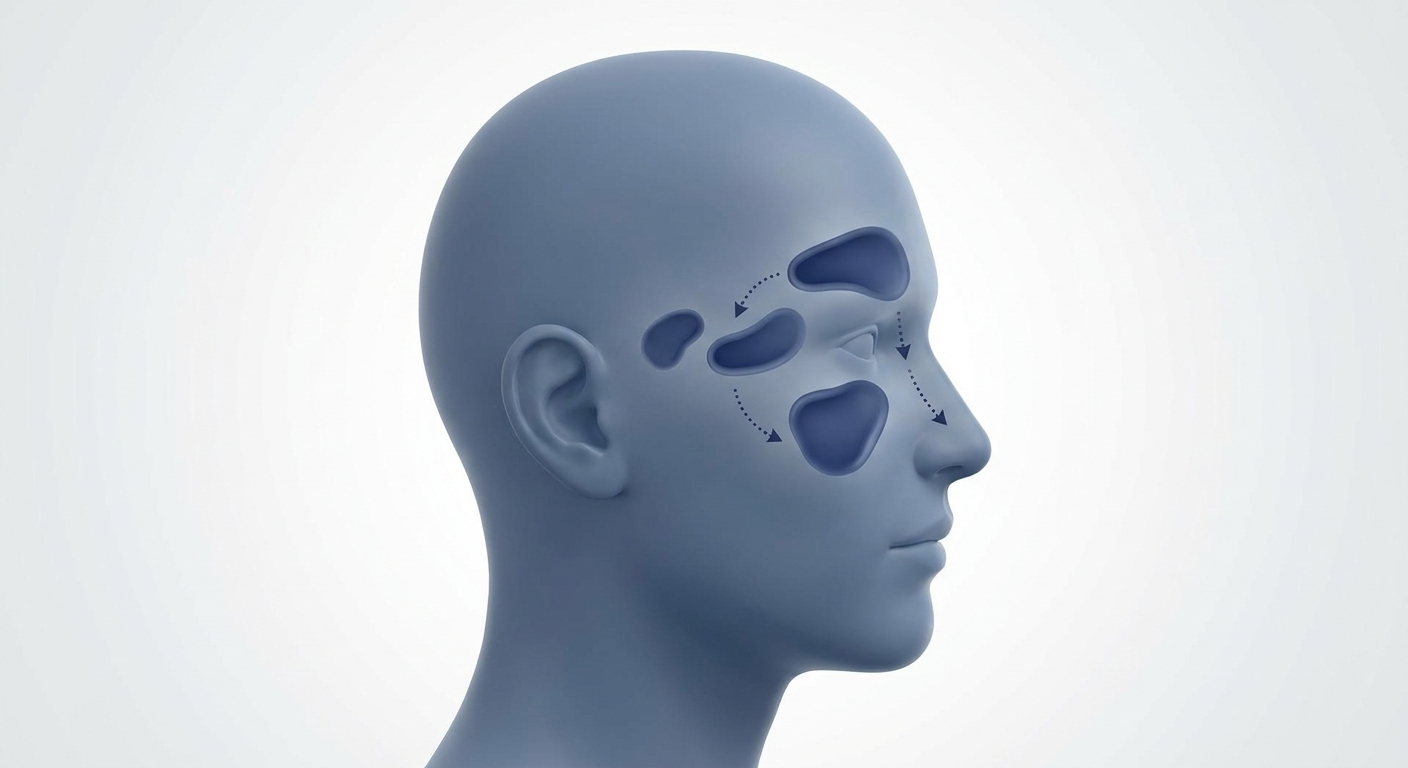
A helpful way to think about it: your sinuses are like small rooms that rely on tiny “doorways” to drain into the nose. When the nasal lining swells (like a hallway getting crowded), those doors don’t drain as well—and pressure, mucus, and discomfort build. Below is a clear, patient-friendly guide to symptoms, causes, viral vs bacterial clues, and evidence-based treatment options.
Many uncomplicated cases improve with time and supportive care tailored to symptoms.
What Is Acute Rhinosinusitis?
Acute rhinosinusitis (ARS) means inflammation of the nasal lining (“rhino-”) and the sinus cavities (“sinusitis”) that lasts less than 4 weeks (“acute”). The combined term matters because the nose and sinuses function like one connected system—when the nasal lining swells, sinus drainage can get blocked too.
Key takeaway: Most uncomplicated cases of acute rhinosinusitis are viral, often following a cold, and many improve with conservative (non-antibiotic) treatments. This timeframe-based definition and diagnostic framework align with AAO-HNS clinical guidance. [2]
Acute rhinosinusitis usually follows a cold and often improves without antibiotics.
Acute Rhinosinusitis vs. the Common Cold vs. “Sinus Infection”
Why symptoms overlap: A cold and acute rhinosinusitis can feel nearly identical at first: inflammation leads to swelling, thicker mucus, and slowed drainage. Because the discomfort centers around the face and nose, many people label any significant congestion a “sinus infection”—even when it’s viral and self-limited.
A common experience sounds like: “My face hurts, my nose is blocked, and the drainage is thick—so it must be bacterial.” In reality, those symptoms can happen in viral illness too, especially during the first week.
If you want a broader symptom checklist, see our sinus symptom overview: https://sleepandsinuscenters.com/symptoms-of-sinus-problems
Acute vs. chronic rhinosinusitis (quick clarity)
- Acute: up to 4 weeks
- Chronic: symptoms persist much longer and usually involve a different evaluation and treatment approach
For a deeper explanation, read our guide on acute vs. chronic rhinosinusitis: https://sleepandsinuscenters.com/blog/acute-vs-chronic-sinusitis-key-differences-and-treatment-options
(AAO-HNS uses this classification system to help standardize diagnosis and care.) [2]
Early on, a bad cold and acute rhinosinusitis often look the same.

Acute Rhinosinusitis Symptoms (What Patients Usually Notice)
Core symptoms doctors look for
- Purulent nasal drainage (thicker/colored drainage from the nose or postnasal drip)
- Nasal obstruction/congestion
- Facial pain/pressure (cheeks, around the eyes, forehead)
These symptom groupings are part of AAO-HNS diagnostic criteria. [2]
To make this more concrete, “facial pressure” can feel like fullness under the eyes, heaviness in the cheeks, or aching around the forehead—sometimes worse when bending forward.
Other common symptoms
- Reduced smell or taste
- Cough (often worse at night due to postnasal drip)
- Ear pressure/fullness
- Fatigue
- Bad breath
One clinician-friendly way to summarize it: when the nose and sinuses are inflamed, it can affect sleep, appetite, and concentration—even if the illness isn’t dangerous.
When symptoms may feel “more severe”
Fever, body aches, and a significant headache can happen—especially early in a viral illness. Severity alone doesn’t automatically mean “bacterial,” which is why timing and symptom pattern matter.
As an ENT might put it: “How long it lasts, and whether it worsens after improving, often tells us more than the color of the mucus.”
A combination of thick drainage, nasal blockage, and facial pressure most strongly points to ARS.
What Causes Acute Rhinosinusitis?
Viral causes (most common)
Most acute rhinosinusitis starts with a typical cold virus. The nasal lining swells, sinus openings narrow, mucus can’t drain well, and pressure builds—leading to classic ARS symptoms. Current ENT-focused reviews emphasize the viral predominance and conservative management for many adults. [1][2]
A simple analogy: inflammation is like a traffic jam. Even if the “road” (your sinus anatomy) is normal, swelling can slow everything down, so mucus lingers longer and feels thicker.
Bacterial causes (less common)
A bacterial infection may develop when blocked drainage persists and bacteria overgrow. However, a common misconception is that colored mucus automatically means bacteria—it doesn’t. Mucus color can change with inflammation and time, even in viral illnesses. Careful diagnosis helps prevent unnecessary antibiotics. [1][2]
In other words, green or yellow drainage can be part of the immune system doing its job; it’s not a stand-alone reason to start antibiotics.
Risk factors that make ARS more likely
- Seasonal allergies or chronic rhinitis
- Recent exposure to upper respiratory infections
- Smoking/vaping or frequent irritant exposure
- Structural blockage (for example, deviated septum or enlarged turbinates)
- Immune compromise (may warrant earlier evaluation because risks and needs can differ)
If you find you’re “always congested” even between colds, that’s a clue to look for ongoing triggers like allergies, irritants, or anatomy.
Mucus color alone doesn’t diagnose bacteria; timing and progression matter more.

Viral vs. Bacterial Acute Rhinosinusitis: How Clinicians Tell the Difference
Clues pointing to viral rhinosinusitis
- Symptoms that peak early and gradually improve over 7–10 days
- Mild-to-moderate discomfort without concerning “red flag” symptoms
For many people, day 2–4 is the roughest stretch, followed by slow improvement. That day-by-day trend is one reason clinicians often recommend supportive care first.
For a more detailed comparison, see: Viral vs bacterial sinus infections: key differences https://sleepandsinuscenters.com/blog/viral-vs-bacterial-sinus-infections-key-differences
When bacterial rhinosinusitis is more likely (“3 classic patterns”)
1) Persistent symptoms that don’t improve (commonly discussed around >10 days)
2) Severe symptoms early in the illness, such as high fever and purulent nasal drainage or facial pain, lasting several days
3) “Double-sickening”: initial improvement followed by a clear worsening again
This persistence/severity/double-worsening framework is highlighted in ENT guidance and reviews. [1][2]
A patient example of “double-sickening” is: “I started to feel better after a week, then two days later I suddenly got worse again—more pressure, thicker drainage, and I felt sicker.”
Testing and imaging—what’s usually not needed
For many adults, diagnosis is based on symptom pattern and timing. CT scans and cultures aren’t routinely needed at the start unless there are complications, unusual features, or recurrent/persistent symptoms that warrant a deeper look.
Persistent, severe, or double‑worsening patterns raise concern for bacteria.
Diagnostic Criteria (What Must Be Present?)
The symptom checklist used in practice
In many settings, acute rhinosinusitis is considered when two or more of the following are present:
- Purulent nasal drainage (front of nose or postnasal drip)
- Nasal obstruction
- Facial pain/pressure
…and the illness duration fits the acute window (up to 4 weeks). [2]
Clinicians also consider the overall story: timing, triggers (like a recent cold), and whether you’re improving, stuck, or clearly worsening.
Why accurate diagnosis matters
When symptoms are viral, antibiotics don’t help—and can cause side effects and contribute to resistance. That’s why modern care emphasizes selecting treatment that matches the likely cause and using antibiotics thoughtfully (antibiotic stewardship). [1][3]
A practical way to frame stewardship is “right treatment, right patient, right time”—not “antibiotics just in case.”
Diagnosis rests on symptom clusters and duration, not scans or mucus color.

Treatment Options for Acute Rhinosinusitis (Evidence-Based and Patient-Friendly)
First-line treatment for most adults: conservative symptom relief
Many guidelines and reviews emphasize supportive care first, especially when a viral cause is likely. [1][3]
1) Saline nasal irrigation
Saline nasal irrigation can help thin mucus, flush irritants, and improve drainage. People often describe it as “resetting” the nose—especially when postnasal drip is triggering cough or throat clearing.
Practical safety points include using sterile/distilled water (or previously boiled and cooled water) and cleaning the device as directed.
For practical frequency guidance, read: how often to use saline nasal rinses https://sleepandsinuscenters.com/blog/nasal-rinses-how-often-should-you-use-them
2) Topical intranasal corticosteroids (nasal steroid sprays)
Intranasal corticosteroids help reduce inflammation and swelling inside the nose, which may improve airflow and drainage—especially when allergies contribute. Evidence-based reviews commonly include them among first-line symptom strategies. [1][3]
If you’re comparing options, this may help: best nasal spray for sinusitis (steroid vs saline vs decongestant) https://sleepandsinuscenters.com/blog/best-nasal-spray-for-sinusitis-steroid-vs-saline-vs-decongestant
Other supportive treatments (when appropriate)
- Pain/fever relief options (as appropriate)
- Hydration and humidified air for comfort
- Rest and sleeping with the head slightly elevated
- Decongestants (used cautiously and typically short-term; topical sprays can cause rebound congestion if overused)
- Antihistamines (more helpful when allergies are a major driver; in some people they can worsen dryness)
A quick “real life” example: if your main issue is pressure and blockage, saline + a nasal steroid may be more useful than an antihistamine—unless sneezing/itching and known allergies are clearly driving symptoms.
When antibiotics may be needed (and when they often aren’t)
Antibiotics are most useful when a bacterial pattern is likely (persistent, severe, or double-worsening). Many uncomplicated cases still resolve without antibiotics, which is why shared decision-making has become standard in many practices. [1][2]
For a deeper discussion, see: Do I always need antibiotics for a sinus infection? https://sleepandsinuscenters.com/blog/do-i-always-need-antibiotics-for-a-sinus-infection
Delayed antibiotic prescription (“watchful waiting” strategy)
A delayed antibiotic prescription is a stewardship approach where a prescription may be provided with instructions to wait and only start it if symptoms worsen or fail to improve after a defined time window. This strategy can reduce unnecessary antibiotic exposure while keeping a safety net in place. It isn’t appropriate for everyone (for example, some immunocompromised patients). [1]
Do antibiotics cure faster? What research suggests
Systematic reviews suggest that many uncomplicated cases improve without antibiotics, and the benefit of immediate antibiotics is often modest; antibiotics are most useful when a bacterial infection is more likely. [1][3]
Start with saline and a nasal steroid when appropriate; reserve antibiotics for likely bacterial cases.
When to See a Doctor (and When It’s Urgent)
Call your provider/ENT if:
- Symptoms last longer than expected, or keep returning
- Facial pain/pressure is significant or worsening
- The illness fits a “double-sickening” pattern
- You have immune suppression or complex medical conditions that may change risk
If you’re unsure whether your symptoms match a viral pattern or a bacterial pattern, a check-in can prevent both undertreatment (missing a bacterial case) and overtreatment (unnecessary antibiotics).
Seek urgent evaluation for red flags
- Swelling/redness around the eye or vision changes
- Severe headache, stiff neck, confusion
- High fever with worsening symptoms
- Facial numbness or severe facial swelling
Know the red flags and seek care promptly if they appear.

Lifestyle Tips to Feel Better and Recover Faster
At-home comfort plan (simple checklist)
- Use a saline rinse once or twice daily if tolerated, following product instructions or a clinician’s guidance
- Use a nasal steroid spray as directed (when recommended)
- Keep up hydration; consider warm showers or properly maintained humidification
- Sleep with the head slightly elevated
- Reduce exposure to smoke, strong fragrances, and known allergens when possible
A small but meaningful tip: nighttime can feel worse because mucus pools when you’re lying flat—so elevating your head slightly can make mornings easier.
Prevention tips (reduce future episodes)
- Hand hygiene and minimizing exposure during peak cold seasons
- Proactive allergy management during pollen seasons
- Address ongoing nasal blockage contributors if symptoms are frequent or persistent
If you’re getting repeated “sinus infections,” prevention often starts with identifying what keeps the nose chronically inflamed between illnesses.
Small daily steps can shorten discomfort and reduce future episodes.
FAQs About Acute Rhinosinusitis
How long does acute rhinosinusitis last? Many cases improve within days to two weeks, and the term acute applies up to 4 weeks. [2]
Is acute rhinosinusitis contagious? When the cause is viral, the virus can spread to others. “Acute rhinosinusitis” describes the inflammation pattern, not a specific virus.
Do I need antibiotics if my mucus is yellow or green? Not necessarily. Mucus color alone doesn’t confirm a bacterial infection; timing and symptom pattern are more meaningful. [1][2]
What’s the best home remedy that’s actually evidence-based? Among the most evidence-supported options are saline nasal irrigation and intranasal corticosteroids for symptom control. [1][3]
Can acute rhinosinusitis turn into chronic rhinosinusitis? Repeated episodes or prolonged inflammation can contribute to ongoing problems. Persistent or recurrent symptoms are a good reason to consider a more detailed evaluation.
Is it safe to use a neti pot? When used correctly (sterile/distilled/boiled water and proper cleaning), it’s generally considered safe. See our neti pot safety tips: https://sleepandsinuscenters.com/blog/neti-pot-safety-tips-essential-steps-for-safe-nasal-irrigation
When in doubt about timing and pattern, check in with a clinician.
When to Consider an ENT Evaluation
Signs you may benefit from a specialist visit
- Recurrent acute rhinosinusitis episodes
- Symptoms not improving with appropriate conservative care
- Ongoing nasal obstruction suggesting structural contributors
- Concern for complications or alternate diagnoses
If episodes are frequent, it’s reasonable to ask, “Is this truly repeated infections—or is something like allergies or nasal blockage setting me up for inflammation every time I catch a cold?”
What an ENT might do differently
- Nasal endoscopy (when indicated)
- A tailored medical plan focused on inflammation control and prevention
- Evaluation of contributing factors such as allergies, anatomy, or chronic inflammation
If episodes repeat or don’t respond, a targeted ENT plan can break the cycle.
Conclusion + Call to Action
Acute rhinosinusitis is common, uncomfortable, and often viral—meaning supportive care like saline nasal irrigation and intranasal corticosteroids may be the main tools for relief, while antibiotics are reserved for cases that fit bacterial patterns. Keeping an eye out for “persistent,” “severe,” or “double-sickening” symptoms—and knowing the red flags—can help guide next steps.
If symptoms persist, worsen, or keep recurring, Sleep and Sinus Centers of Georgia can help you sort out whether this is acute rhinosinusitis, allergy-driven inflammation, structural blockage, or something else—and discuss appropriate treatment options. To book an appointment, visit https://www.sleepandsinuscenters.com/ and choose a convenient time.
The right treatment at the right time makes all the difference.
References
1. Otorhinolaryngology Poland (2023). Acute rhinosinusitis overview and management trends. https://otorhinolaryngologypl.com/article/142023/en
2. American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) (2021). Adult Sinusitis: Diagnostic Criteria for Rhinosinusitis (PDF). https://www.entnet.org/wp-content/uploads/2021/04/adult-sinusitis-physicianresource-diagnostic-criteria-rhinosinusitis.pdf
3. Otolaryngology–Head and Neck Surgery (AAO-HNSF) journal summary. Rhinosinusitis management guidance and evidence considerations. https://aao-hnsfjournals.onlinelibrary.wiley.com/doi/10.1002/ohn.1344
Medical Disclaimer
This article is for educational purposes only and does not replace individualized medical advice. If you have severe symptoms or urgent red flags, seek prompt medical care.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.