Sinus Disease in Long-Term Steroid Users: Symptoms, Risks, and Treatment
If you’ve ever felt instant relief from a course of prednisone—only to have congestion, pressure, and drainage return soon after the last pill—you’re not imagining things. That “better on steroids, worse off steroids” cycle is common in chronic inflammatory sinus conditions. Many patients describe it the same way: “By day three I can finally breathe again… then a week after I stop, it’s right back.” This rebound often suggests persistent inflammation rather than a resolved infection. In many cases, this pattern points to steroid-dependent sinus disease, a form of chronic rhinosinusitis (CRS) where steroids temporarily calm inflammation but don’t fully control what’s driving it. Instead of a one-time infection, it’s often an ongoing inflammatory process that needs a long-term plan. The goal is steady symptom control with less reliance on systemic (whole-body) steroids, using “steroid-sparing” strategies that focus on topical therapy, identifying triggers, and targeted treatments. [1][2]
Important safety note
Seek urgent evaluation right away if you notice:
- Swelling around the eye or vision changes
- Severe headache with fever or stiff neck
- Neurologic symptoms or confusion
- Rapid worsening in immunosuppressed patients, including those on long-term systemic steroids
What “Steroid-Dependent” Sinus Disease Means
The classic pattern patients notice
Steroid-dependent CRS often follows a familiar timeline:
- Symptoms improve significantly during an oral steroid burst or taper
- Symptoms rebound days to weeks after finishing
- The cycle repeats with the next flare
Systemic steroids can temporarily “turn down the volume” on inflammation, but if the underlying driver is still active, symptoms often return as soon as the medication is gone. That rebound suggests persistent inflammation, not simply a sinus infection that was cured. This is a clinical pattern observed in some patients and is not a universally formal diagnosis everywhere. [1]
Steroids treat inflammation—but don’t always fix the cause
Systemic steroids can be powerful at reducing swelling and mucus—but they may also mask underlying drivers such as:
- Allergies
- Nasal polyps
- Structural blockage (narrow drainage pathways, septal deviation)
- Non-allergic inflammation or irritant sensitivity
If any of these are present, prednisone may provide short-term relief, but the “why” behind the inflammation remains. For a deeper explanation of this pattern, see Sleep and Sinus Centers of Georgia’s overview of steroid-dependent sinus disease: https://sleepandsinuscenters.com/blog/steroid-dependent-sinus-disease-causes-symptoms-an-20260206191202. [1]
Bottom line: Fast relief on steroids with quick relapse off them often points to ongoing inflammation that needs a longer-term plan.

Symptoms to Watch For (When Steroids Are Wearing Off)
Common chronic rhinosinusitis symptoms
CRS symptoms can be steady, or they can fluctuate as steroids start and stop:
- Nasal congestion or obstruction
- Facial pressure/fullness
- Thick drainage or post-nasal drip
- Reduced smell or taste
- Cough, throat clearing
- Fatigue, poor sleep
It’s not unusual for people to notice their sleep quality track with their nasal symptoms—when the nose is blocked, mouth breathing increases, dryness worsens, and sleep becomes lighter or more fragmented. If symptoms persist beyond 12 weeks, it may fit the definition of CRS (sometimes referred to as chronic sinusitis): https://sleepandsinuscenters.com/chronic-sinusitis. [2]
Symptoms that often suggest nasal polyps or severe inflammation
- Marked loss of smell (especially persistent)
- Ongoing blockage despite rinses and sprays
- Recurring flare-ups that repeatedly require steroid bursts
Polyps and inflammatory CRS frequently drive steroid-rebound patterns. Learn more about nasal polyps and how they affect airflow and drainage: https://sleepandsinuscenters.com/blog/what-are-nasal-polyps. [2]
If symptoms last beyond 12 weeks or rebound after steroids, think chronic inflammation, not just infection.

Why Long-Term Systemic Steroids Are Risky (And Usually Avoided)
“Systemic” means pills or injections that affect the whole body.
Key long-term risks clinicians worry about
- High blood sugar/diabetes risk
- Osteoporosis and fracture risk
- Cataracts
- Adrenal suppression (the body reduces its own steroid production)
- Growth suppression in children
Even repeated short courses can add up
Even “just a few bursts” per year can create meaningful cumulative exposure. Over months and years, the pattern can become a cycle: flare → steroid burst → rebound → flare. That cycle signals it’s time to look for longer-term control rather than repeating the same short-term fix. [1][2]
When systemic steroids may still be used
In some cases, systemic steroids are used as a short-term bridge for severe inflammation (often with polyps), especially while initiating longer-term strategies like topical regimens, procedures, or biologics—always under clinician guidance. [2]
Goal: control sinus inflammation while minimizing whole-body steroid exposure.

Common Causes & Drivers in Steroid-Dependent Sinus Disease
Nasal polyps and type 2 inflammation
Polyps can physically block airflow and drainage and are often linked to type 2 inflammation. Symptoms may improve dramatically on systemic steroids, then quickly return without ongoing anti-inflammatory control. If polyps block key drainage pathways, sprays may not reach the areas that need medication most—so inflammation quiets down briefly with prednisone, then ramps back up. [2]
Allergic rhinitis (seasonal or perennial)
Allergies can continuously fuel nasal and sinus inflammation. Identifying triggers can help guide targeted treatment choices. Learn more about allergy testing: https://sleepandsinuscenters.com/allergy-testing. [3]
Non-allergic inflammation/irritant sensitivity
Irritants such as smoke, strong fragrances, pollution, and workplace exposures can provoke symptoms that mimic allergies and keep inflammation smoldering. For some patients, this looks like “random” flares—symptoms spike after a trigger exposure, improve temporarily on steroids, then return because the underlying sensitivity is still present.
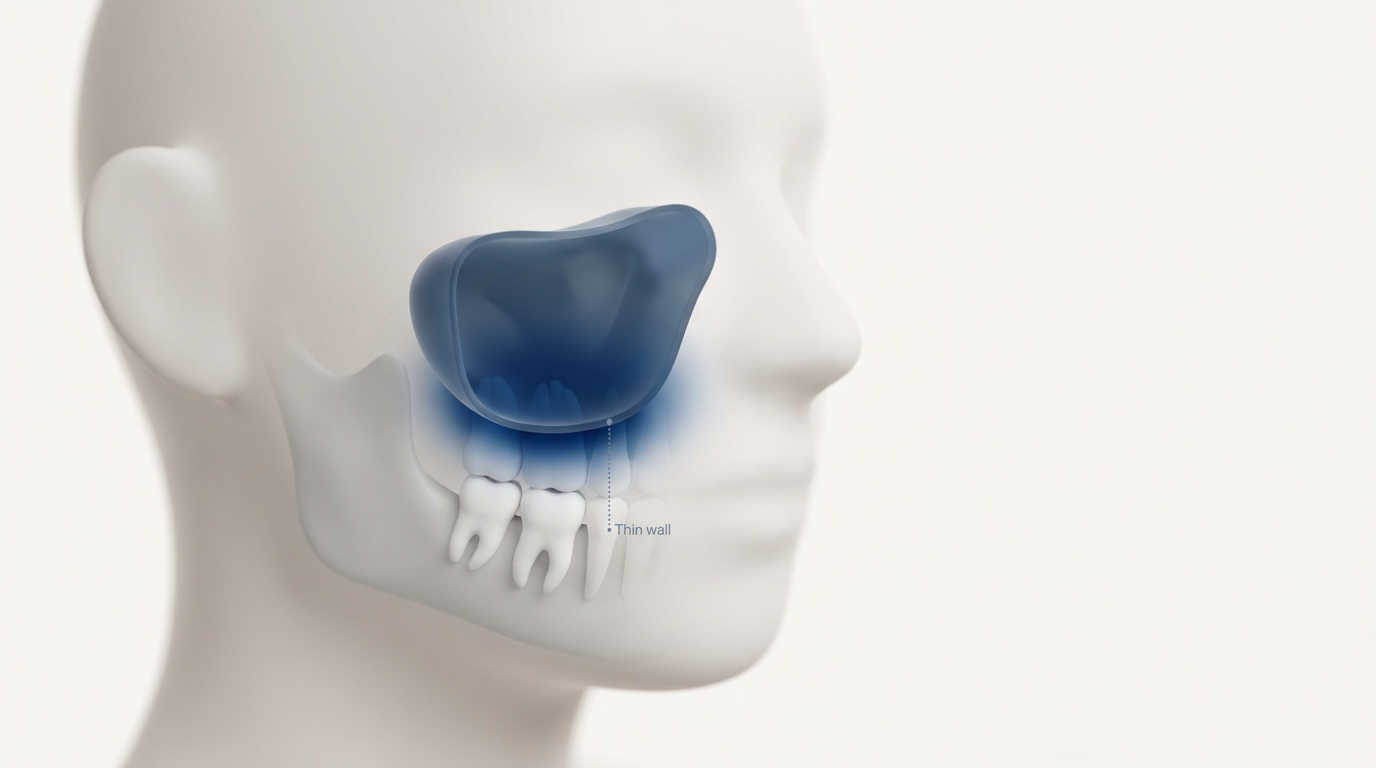
Structural blockage
Anatomy can play a role (deviated septum, turbinate hypertrophy, narrow drainage pathways). Structural issues can also reduce how well topical medications reach inflamed areas—one reason some patients struggle with sprays alone. [2]
Treating the driver reduces the need for rescue steroids.
How ENT Specialists Diagnose the Problem (Beyond “Just Take Steroids”)
History that signals steroid dependence
- How many steroid courses you’ve needed per year
- How fast symptoms rebound after stopping
- Smell loss, polyp history
- Asthma or aspirin-exacerbated respiratory disease (AERD) history
Nasal endoscopy (in-office)
Endoscopy helps visualize inflammation, polyps, drainage/mucus, and anatomical narrowing. Seeing the nasal cavity directly can help distinguish chronic inflammation-driven symptoms from issues that look like infection but behave more chronically.
CT scan of the sinuses
A CT scan maps where inflammation and blockage are occurring and can help guide medical vs procedural decisions: https://sleepandsinuscenters.com/blog/sinus-ct-scan-what-it-shows-and-how-it-helps-diagnose-sinus-issues. [2]
Checking for underlying contributors
Depending on symptoms, the workup may include allergy evaluation and, in select cases, consideration of immune or systemic inflammatory conditions. [2]
A clear diagnosis guides safer, more effective long-term care.

Steroid-Sparing Treatments (Safer Long-Term Control)
Step 1 — Optimize topical steroid therapy (the foundation)
For many patients, consistent topical treatment is the cornerstone of steroid-sparing care:
- Daily topical nasal steroids (intranasal corticosteroid sprays)
- High-volume saline rinses to help clear mucus and improve medication delivery
Technique matters. If sprays haven’t helped, it may be worth reviewing proper nasal steroid spray technique to improve results without increasing systemic exposure: https://sleepandsinuscenters.com/blog/steroid-nasal-spray-technique-step-by-step-guide-for-effective-use. In some cases, ENTs may recommend steroid mixed into irrigations for a more localized effect: https://sleepandsinuscenters.com/blog/steroid-rinses-a-modern-approach-to-sinus-relief. [2]
Step 2 — Treat the driver(s)
- Allergy management: antihistamines (when appropriate), environmental controls, and immunotherapy options for selected patients [3]
- Nasal polyps management: topical strategies and escalation pathways when needed [2]
- Irritant reduction: avoid smoke/fragrance exposures when possible
Step 3 — Medications that may reduce inflammation without systemic steroids
- Antibiotics when bacterial infection is likely (rather than reflexively). Antibiotics are ineffective if symptoms are purely inflammatory, and use should be guided by clinical evaluation to avoid unnecessary use.
- Leukotriene modifiers for selected patients
- Other anti-inflammatory approaches matched to the pattern of disease [2]
Step 4 — Biologic therapies (for appropriate CRS patients, often with polyps)
Biologics are targeted injectable medications designed to interrupt specific inflammatory pathways. They’re typically considered for severe CRS with nasal polyps, especially when symptoms persist despite strong topical therapy, when systemic steroids are repeatedly needed, or after prior surgery—under specialist guidance following thorough evaluation. [2]
Step 5 — Procedures/surgery (when blockage limits control)
When polyps or anatomy block drainage—or prevent topical medications from reaching key areas—procedures may be discussed. Endoscopic sinus surgery can improve ventilation and help topical treatments work better in the long term. Surgical decisions are individualized and should be discussed with an ENT specialist. (Some patients may also discuss balloon-based approaches depending on anatomy and disease pattern.) [2]
Emerging research: reducing steroid resistance
Research continues into why some CRS becomes less responsive to steroids and how newer treatments may improve long-term control while reducing systemic exposure. [2]
Consistent topical care plus driver-focused therapy is the backbone of steroid-sparing control; advanced options are specialist-guided.

Lifestyle Tips to Reduce Flares (Practical, Patient-Friendly)
Daily sinus-care routine (simple checklist)
- Saline rinse + prescribed topical spray (as directed)
- Keep indoor air from getting overly dry
- Reduce triggers (smoke, strong fragrances, dust/mold)
Allergy-smart habits
- Shower after outdoor exposure on high-pollen days
- Bedroom controls (HEPA filtration, wash linens regularly)
- Keep pets out of the bed if sensitivity is suspected
Infection prevention basics
- Hand hygiene
- Address reflux if it’s a known contributor to throat symptoms
- Avoid overusing topical decongestant sprays (they can cause rebound congestion)
Small, steady habits help prevent big flares.
When to See an ENT (Especially if You’re Using Steroids Often)
Consider evaluation if you have any of the following:
- Repeated oral steroid bursts for sinus symptoms
- Smell loss that doesn’t recover
- Symptoms lasting more than 12 weeks or frequent recurrences [2]
- Suspected polyps, asthma/AERD, or major sleep disruption
- Side effects from steroids (bone, glucose, or eye issues)
What to bring to your appointment
- A medication list with steroid doses/dates
- Prior CT/endoscopy reports if available
- A symptom timeline, especially rebound timing
If you keep needing steroid bursts, it’s time to discuss a steroid-sparing plan.
FAQs
Is it safe to be on oral steroids long-term for sinus problems?
Long-term systemic steroids are generally discouraged for chronic rhinosinusitis because of meaningful whole-body risks. Many care plans emphasize steroid-sparing strategies for safer long-term control. [2][3]
Why do my sinus symptoms come back as soon as I stop prednisone?
A quick rebound after stopping steroids often indicates persistent inflammation—commonly called steroid-dependent CRS—rather than a condition that has fully resolved. [1][2]
Are nasal steroid sprays safer than oral steroids?
Typically yes. Topical nasal steroids mainly target the nasal lining with less whole-body exposure than oral steroids, especially when used correctly and consistently. [2]
What treatments can reduce my need for steroid bursts?
Options may include optimized topical therapy (sprays/rinses), addressing allergies and polyps, evaluating structural blockage, and—when appropriate—biologics or sinus procedures/surgery. Such treatments should be considered under specialist guidance after thorough evaluation. [2][3]
When are antibiotics helpful?
Antibiotics are most helpful when a bacterial infection is likely. Many chronic symptoms in CRS are driven more by inflammation than infection, so antibiotic decisions should be based on clinical evaluation to avoid overuse. [2]
Conclusion / Next Steps
Sinus disease in long-term steroid users often reflects chronic inflammation that temporarily responds to systemic steroids but rebounds when they stop. Because long-term systemic steroids carry real risks, many patients do better with a steroid-sparing treatment plan: optimized topical nasal steroids, identification of drivers like allergies or polyps, and targeted therapies—including biologics or procedures when needed. If your symptoms follow the steroid-rebound pattern, Sleep and Sinus Centers of Georgia offers educational and evaluation resources, including the sinus symptom quiz (https://sleepandsinuscenters.com/sinus-symptom-quiz). If you’re relying on repeated steroid bursts (or trying to avoid them), you can also book an appointment to discuss a longer-term plan tailored to your symptoms and risk factors (https://sleepandsinuscenters.com/appointments). [1][2]
Lasting control usually comes from addressing the cause, not repeating short-term fixes.
References
[1] Sleep and Sinus Centers of Georgia. Steroid-Dependent Sinus Disease: Causes, Symptoms, and… https://sleepandsinuscenters.com/blog/steroid-dependent-sinus-disease-causes-symptoms-an-20260206191202
[2] NCBI / PubMed Central. Review on CRS inflammation and management, including steroid-sparing strategies and emerging therapies. https://pmc.ncbi.nlm.nih.gov/articles/PMC6941282/
[3] PubMed (2018). CRS and steroid use considerations (systemic steroid risks/approach). https://pubmed.ncbi.nlm.nih.gov/29059082/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.