Newborn Deviated Septum: Symptoms, Causes, and Treatment Options
Introduction: Why nasal breathing matters in newborns
Newborns preferentially breathe through their noses, which is especially important during feeding and sleep. In the first weeks of life, even mild newborn nasal obstruction can look dramatic: noisy “snorty” breathing, frequent pauses while eating, or restless sleep that improves only when a baby briefly cries (because the mouth opens).
The reassuring news is that many cases of newborn deviated septum are mild and temporary, but severity can vary. Still, some babies develop enough blockage to affect breathing and feeding, and those cases may benefit from prompt evaluation and (in select situations) early correction.
Educational note: This article is for general information and isn’t a substitute for medical care. If you’re concerned about a baby’s breathing or feeding, a clinician who can examine your child is the best next step.
What is a deviated septum in a newborn?
The nasal septum (simple anatomy)
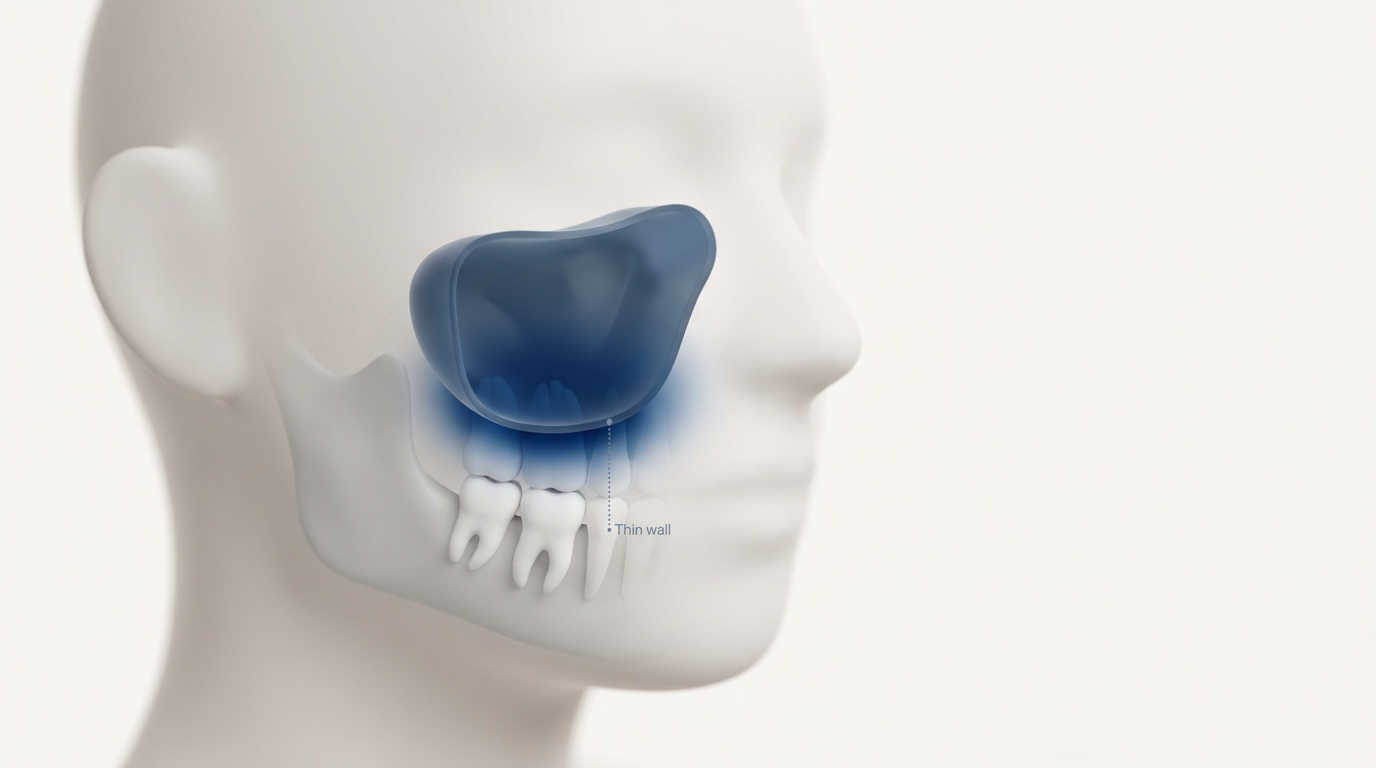
The nasal septum is the thin wall of cartilage and bone that divides the nose into two nostrils. When the septum shifts off-center, one nasal passage becomes narrower. Clinicians call that a “deviated septum.”
A simple way to picture it: if the septum is like the divider in a two-lane tunnel, a shift to one side makes one “lane” tight and the other roomier—so airflow is uneven.
If you’d like a broader overview beyond newborns, see our guide on what a deviated septum is: https://sleepandsinuscenters.com/blog/what-is-a-deviated-septum-causes-symptoms-and-when-to-see-a-doctor

Deviated septum vs. “newborn congestion”
Many newborns sound congested, even when they’re otherwise healthy. Normal newborn congestion often fluctuates—better at some times of day, worse at others—and commonly improves with time and routine supportive care.
In contrast, deviated septum in newborns may be more likely to cause:
- Persistent one-sided blockage
- A consistently “tight” nostril on one side
- Visible asymmetry in the nose shape (what some parents describe as a crooked newborn nose)
That said, congestion and septal deviation can overlap—swelling and mucus can make a mild deviation seem worse for a few days.
Many “snorty” newborns simply have temporary congestion, but a persistently tighter side or visible asymmetry can be a clue to septal deviation.

How common is a newborn deviated septum?
Reported incidence varies widely (and why)
Medical studies report a wide range—approximately 0.08% to 31%—because researchers use different definitions and different exam methods (Harugop et al., 2011; Erdoğdu, 2022; Podoshin et al., 1991). Many prospective studies land around 10–20%, while studies using narrower criteria report under 1%.
In other words, the number changes depending on how strictly deviation is defined and how carefully babies are examined. Some studies count any visible shift, while others count only deviations thought to cause meaningful obstruction.
- Harugop et al., 2011 (PMC)
- Erdoğdu, 2022 (Istanbul Medical Journal)
- Podoshin et al., 1991 (PubMed)
Takeaway for parents
A newborn deviated septum is not rare, and most cases are not dangerous. The most important question isn’t the label—it’s whether symptoms suggest meaningful obstruction, especially around feeding and breathing.
Incidence numbers vary, but what matters most is how well your baby breathes and feeds.
Causes and risk factors (what research shows)
Birth-related mechanical forces (most common explanation)
Many cases of neonatal septal deviation are linked to mechanical forces during labor and delivery—particularly when delivery is difficult or requires assistance. Research has found higher rates associated with factors such as (Harugop et al., 2011; Erdoğdu, 2022):
- Instrument-assisted delivery (forceps or vacuum)
- Emergency cesarean
- First-born status (primiparity)
- Higher birth weight (an association, not necessarily a cause)
These associations support the idea that some deviations reflect “molding” or pressure effects around birth. You may even hear clinicians describe this as the nose being “pushed” or “molded” during delivery.
Congenital vs. birth-related: does it matter?
Often, it does—at least for expectations. Many newborn deviations are thought to be related to birth molding or minor trauma and may improve as swelling resolves and tissues settle. A smaller subset is more structural and may persist.
A practical way to think about it: some deviations behave like a temporary “bend” in soft cartilage right after delivery, while others behave more like a fixed shift that doesn’t self-correct as easily.
Less common considerations
Not all nasal blockage is a deviated septum. Other causes of newborn nasal obstruction can include:
- Swelling after delivery
- Thick mucus
- Less common congenital nasal differences
Because causes can overlap, persistent symptoms are a good reason to seek an exam rather than guessing.
Many deviations relate to birth molding and improve, but persistent symptoms warrant a careful exam.
Symptoms of deviated septum in newborns (what parents may notice)
Breathing signs
Parents may notice:
- Noisy nasal breathing (“snorting”)
- Ongoing stuffiness that seems worse on one side
- Signs of increased work of breathing, such as nasal flaring or chest retractions
A helpful detail to watch for is consistency. If the same nostril always seems more blocked—during feeds, during sleep, and even after gentle supportive care—that pattern can be a clue.
Feeding-related symptoms (a big clue)
Feeding is often where nasal obstruction shows up most. Babies coordinate sucking, swallowing, and breathing—and nasal airflow matters. When obstruction is significant, some infants may have (Harugop et al., 2011; Erdoğdu, 2022):
- Trouble latching or staying latched
- Frequent pauses during feeds to breathe
- Fatigue during feeding or difficulty finishing feeds
- Slower weight gain (when feeding efficiency is affected)
One way clinicians sometimes summarize it is: “If a newborn can’t breathe comfortably through the nose, feeding can turn into a stop-and-start workout.”

Visible appearance changes
Some infants have visible asymmetry, such as:
- A nose that looks shifted to one side
- Uneven nostrils
- A tip that points slightly off-center
A visible “crooked” appearance doesn’t always mean serious blockage, but it can be a useful clue for clinicians evaluating a possible newborn deviated septum.
What this can look like in real life
For example, a parent might notice that photos taken right after delivery show the nose leaning to one side, and the baby consistently sounds noisier when lying on their back. Another family might report feeds taking much longer because the baby unlatches to “catch a breath,” especially when the more blocked side seems compressed.
Consistent one-sided blockage, feeding challenges, and visible asymmetry are common real-world clues.
When to seek urgent care vs. schedule an ENT visit
Seek urgent evaluation (same day/ER) if you notice
Because newborns have small airways and limited reserve, breathing concerns deserve prompt attention. Educational red flags often include:
- Blue color around lips or face (cyanosis)
- Significant breathing distress (retractions, persistent flaring)
- Repeated choking or inability to feed with fewer wet diapers
- Any episode of apnea (pauses in breathing)
If you are ever unsure about your infant’s breathing or feeding, seek prompt medical evaluation.
Schedule early ENT assessment when
An early exam can be helpful when:
- Feeding is consistently difficult
- One-sided blockage persists beyond expected “newborn stuffiness”
- There is visible nasal deformity noted after delivery
For additional guidance on timing and triage, see when you should see an ENT: https://sleepandsinuscenters.com/blog/when-should-i-see-an-ent. Symptomatic infants are commonly highlighted in the literature as appropriate for early assessment (Harugop et al., 2011; Erdoğdu, 2022).
Urgency is driven by symptoms—err on the side of being seen if there’s any concern.

How doctors diagnose a deviated septum in a newborn
What the exam may include
Diagnosis is usually clinical and may involve:
- External inspection of nasal shape and symmetry
- A gentle internal look at the front of the nose (anterior rhinoscopy)
- In specialty settings, a clinician may consider nasal endoscopy to better understand the inside of the nasal passages when the cause of obstruction isn’t clear: https://sleepandsinuscenters.com/blog/what-is-nasal-endoscopy----and-is-it-painful
The goal is to separate a structural narrowing (like a deviated septum) from temporary swelling and mucus that can mimic it.
Why imaging usually isn’t needed
Imaging is not commonly required for straightforward cases. Most suspected septal deviations in newborns can be assessed through history and physical exam. Imaging is more often reserved for unusual presentations or complex obstruction concerns.
Questions your clinician may ask
To understand possible causes and severity, clinicians often ask about:
- Delivery details (prolonged labor, instrument use)
- Breathing patterns and sleep sounds
- Feeding duration and breaks during feeding
- Weight trends and diaper counts
These practical details help connect “what the nose looks like” with “how the baby is doing.”
A hands-on exam and careful history are usually enough to clarify the cause and severity.
Treatment options (from conservative care to early bedside correction)
Option 1 — Watchful waiting (for mild or improving cases)
Many mild deviations improve without a procedure as swelling decreases and the nose continues to develop (Harugop et al., 2011; Erdoğdu, 2022). In these situations, clinicians often focus on monitoring feeding, breathing, and growth.
If your baby is feeding efficiently, staying comfortable at rest, and gaining weight appropriately, careful observation is often a reasonable plan.
Option 2 — Supportive care to reduce obstruction symptoms
Supportive measures may be used to help reduce symptoms while the baby is observed, such as:
- Saline nasal drops/spray as recommended by your pediatrician to avoid irritation or accidental overuse (including the rare risk of water intoxication)
- Gentle suctioning (over-suctioning can irritate delicate tissue)
- Humidified air and practical feeding-position strategies, as advised by a pediatric clinician
Supportive care won’t “move” the septum, but it can reduce the added obstruction from mucus and irritation—sometimes enough to make feeding and sleep noticeably easier.
Option 3 — Early bedside closed reduction (48–72 hours window)
In selected cases—especially when deviation is significant and symptoms suggest meaningful obstruction—some centers report good outcomes with closed-reduction techniques performed in the first 48–72 hours after birth (Harugop et al., 2011; Erdoğdu, 2022). In plain language, “closed reduction” means a trained clinician gently repositions the septum closer to the midline without an incision.
Important context:
- This procedure is not standard for all cases and is not available everywhere.
- It should only be performed by specialists in appropriate settings.
- It is typically brief and well tolerated, with monitoring and follow-up.
What about surgery (septoplasty) in infancy?
A formal operative septoplasty in a newborn is uncommon and generally not first-line. Surgical correction is usually reserved for persistent, symptomatic cases that do not improve with time and supportive care, often reassessed later in childhood.
For a broader overview of care pathways, visit deviated septum relief options: https://sleepandsinuscenters.com/deviated-septum-relief
Mild cases often improve with time; selected symptomatic cases may benefit from specialist-directed early correction.

What to expect if your baby needs early closed reduction
Timing and why early matters
Early reduction is often discussed because newborn cartilage is more malleable shortly after birth, which may make repositioning easier during that early window (Harugop et al., 2011; Erdoğdu, 2022). This is also why clinicians may recommend evaluation sooner rather than later when symptoms are significant.
Comfort and safety (high-level, parent-friendly)
When performed, the procedure is typically brief, and babies are monitored. Families are usually given follow-up instructions and what to watch for afterward (for example, worsening blockage or bleeding), with a plan for recheck.
A parent-focused way an ENT clinician might summarize the goal is: “We’re trying to restore airflow early so feeding and breathing are easier—then we follow closely to be sure things stay on track.”
Follow-up and longer-term monitoring
Follow-up generally focuses on practical outcomes:
- Is breathing quieter/easier?
- Is feeding more efficient?
- Are weight and growth tracking appropriately?
- Does nasal airflow seem more symmetric over time?
The goal is safer, easier breathing and feeding now, and steady progress over time.
Long-term outlook (prognosis)
Most newborns do well
The overall outlook is favorable. Many mild cases improve on their own, and symptomatic cases treated early often show durable improvement in published reports (Harugop et al., 2011; Erdoğdu, 2022).
Potential downstream issues if significant obstruction persists
If meaningful obstruction continues, some children may develop ongoing mouth-breathing, sleep disruption, or chronic nasal blockage. Those symptoms can be addressed over time with pediatric and ENT follow-up, tailored to the child’s age and development.
Most babies do well; persistent symptoms can be managed with ongoing care.
Practical at-home tips for parents (safe, supportive steps)
Feeding tips when nasal breathing is harder
If a baby tires easily during feeds, some families find it helpful (in coordination with a pediatric clinician or lactation support) to:
- Offer shorter, more frequent feeds
- Build in brief breathing breaks
If you notice your baby consistently “works” to feed—pausing often, getting sweaty or fussy, or taking an unusually long time—bring those details to your clinician. They help guide next steps.
Keep nasal passages as clear as possible
- Use saline only as recommended for infants (ask your pediatrician).
- Suction gently and sparingly to avoid irritation.
Sleep and environment
- Follow safe sleep guidance (back to sleep; avoid unsafe positioning devices).
- Reduce irritants like smoke, strong fragrances, and excess dust.
Simple, gentle steps—plus close attention to feeding—can make a meaningful difference at home.
FAQs (SEO-friendly, patient-focused)
Can a newborn be born with a deviated septum?
Yes. A newborn deviated septum may be present at birth, often linked to molding or pressure during delivery, though some cases may be more structural.
Is a deviated septum in a newborn an emergency?
Not always. The urgency is driven by symptoms—especially breathing distress or feeding problems. Any signs of significant respiratory difficulty warrant prompt evaluation.
How can I tell the difference between a deviated septum and normal newborn congestion?
Congestion tends to fluctuate. A septal deviation is more likely to cause persistent one-sided obstruction or visible asymmetry.
Will a newborn deviated septum fix itself?
Many mild cases may improve spontaneously (Harugop et al., 2011; Erdoğdu, 2022).
What causes a crooked nose after birth?
A “crooked” appearance can be related to birth forces, with higher rates reported after difficult or instrument-assisted deliveries in some studies (Harugop et al., 2011; Erdoğdu, 2022).
When should closed reduction be done?
When it’s considered appropriate, literature often cites a 48–72 hour window for early bedside reduction (Harugop et al., 2011; Erdoğdu, 2022). Not all centers offer this, and not all babies need it.
Is closed reduction painful or risky?
Reports commonly describe it as brief and well tolerated when performed by trained clinicians in appropriate settings, with monitoring and follow-up. Individual risk depends on the baby’s situation and should be discussed during evaluation.
Could a deviated septum affect breastfeeding or bottle-feeding?
Yes. Significant obstruction can interfere with coordinated breathing during feeds, which may lead to fatigue, pauses, and inefficient feeding (Harugop et al., 2011; Erdoğdu, 2022).
Will my child need septoplasty later?
Most infants will not. If symptoms persist as a child grows, ENT evaluation can help determine whether any later intervention is needed.
Which specialist treats newborn deviated septum—pediatrician or ENT?
Pediatricians often identify the concern and assess overall health and feeding. An ENT specialist may evaluate anatomy and discuss options when symptoms or visible deformity suggest meaningful obstruction.
Conclusion and next steps
A newborn deviated septum can look alarming, but many cases are mild and improve. What matters most is how your baby is doing—breathing comfortably, feeding efficiently, and growing well.
If there’s persistent one-sided blockage, visible nasal asymmetry, or feeding and breathing difficulty, an early evaluation can clarify whether this is simple newborn congestion or a more significant neonatal septal deviation that may benefit from closer follow-up or early correction (Harugop et al., 2011; Erdoğdu, 2022). To talk through symptoms and next steps, book an appointment with Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
Early, symptom-focused evaluation helps ensure your baby breathes and feeds as comfortably as possible.
References
- Harugop AS et al. (2011). Neonatal nasal septal deviation—Incidence and etiology. Indian Journal of Otolaryngology and Head & Neck Surgery. https://pmc.ncbi.nlm.nih.gov/articles/PMC3431516/
- Erdoğdu S. (2022). Septal deviation in newborns: A prospective study and literature review. Istanbul Medical Journal. https://www.istanbulmedicaljournal.org/articles/septal-deviation-in-newborns-a-prospective-study-and-literature-review/doi/imj.galenos.2022.01212
- Podoshin L. et al. (1991). Incidence and treatment of nasal septal deviations in newborns. Ear Nose Throat Journal. https://pubmed.ncbi.nlm.nih.gov/1935710/
- Background sources cited historically in neonatal septal deviation literature include Tasca & Compadretti (2004) and Gray (1978).
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.