Nasal Valve Collapse: Symptoms, Causes, and Treatment Options
If you struggle to breathe through your nose—especially during deep breaths, exercise, or sleep—you may have heard terms like “deviated septum” or “allergies.” Another common (and often overlooked) cause is nasal valve collapse. Because the nasal valve area is the narrowest “bottleneck” in the nasal airway, even small changes there can create big symptoms. [1,2]
Think of nasal airflow like water moving through a hose: if the hose is pinched at its narrowest point, it doesn’t matter much if the rest of the hose is wide open—you’ll still feel the restriction. That’s why nasal valve issues can feel dramatic, especially when you’re trying to pull more air in (exercise, anxiety, a stuffy night of sleep). [1,2]
This guide explains what nasal valve collapse is, how ENTs evaluate it, and what treatment options may help—from simple supports to office procedures and functional nasal surgery.

What Is Nasal Valve Collapse?
In patient-friendly terms, nasal valve collapse happens when the narrowest part of the nasal airway becomes too weak or too narrow and pinches inward, making it harder to move air through your nose.
A quick “bottleneck” analogy (why it feels worse with deep breaths): During a gentle breath, a mildly narrow valve may be good enough. But when you inhale more forcefully, the airflow demand rises—and the soft tissues can pull inward (dynamic collapse), making obstruction feel suddenly worse. This is why many people say, “I can breathe okay at rest, but not when I’m exercising,” or “My nose feels like it closes when I sniff in.” [1,2]
Why it’s commonly missed: Nasal breathing problems are frequently attributed to a deviated septum, turbinate enlargement, or rhinitis (allergic/nonallergic inflammation). Those issues can absolutely matter—but if the valve is the main bottleneck, treating only the septum or turbinates may not fully resolve symptoms.
In some patients, septoplasty alone may not fully relieve symptoms if nasal valve dysfunction is also present. Reported rates of persistent symptoms after septoplasty vary across studies, and some series report rates in the range of approximately 19% to 50%. [2]
Why the nasal valve matters for breathing: The nasal valve region strongly influences airflow and nasal resistance. Because it’s already narrow, relatively small anatomical narrowing—or weakness that allows inward collapse during inhalation—can lead to noticeable obstruction. [1,2]
In short: small changes at the valve can have big breathing effects.

Nasal Valve Anatomy (Internal vs External)
Understanding where the airway is narrowing helps explain why treatments differ. Clinicians often separate valve problems into the internal nasal valve (INV) and external nasal valve (ENV).
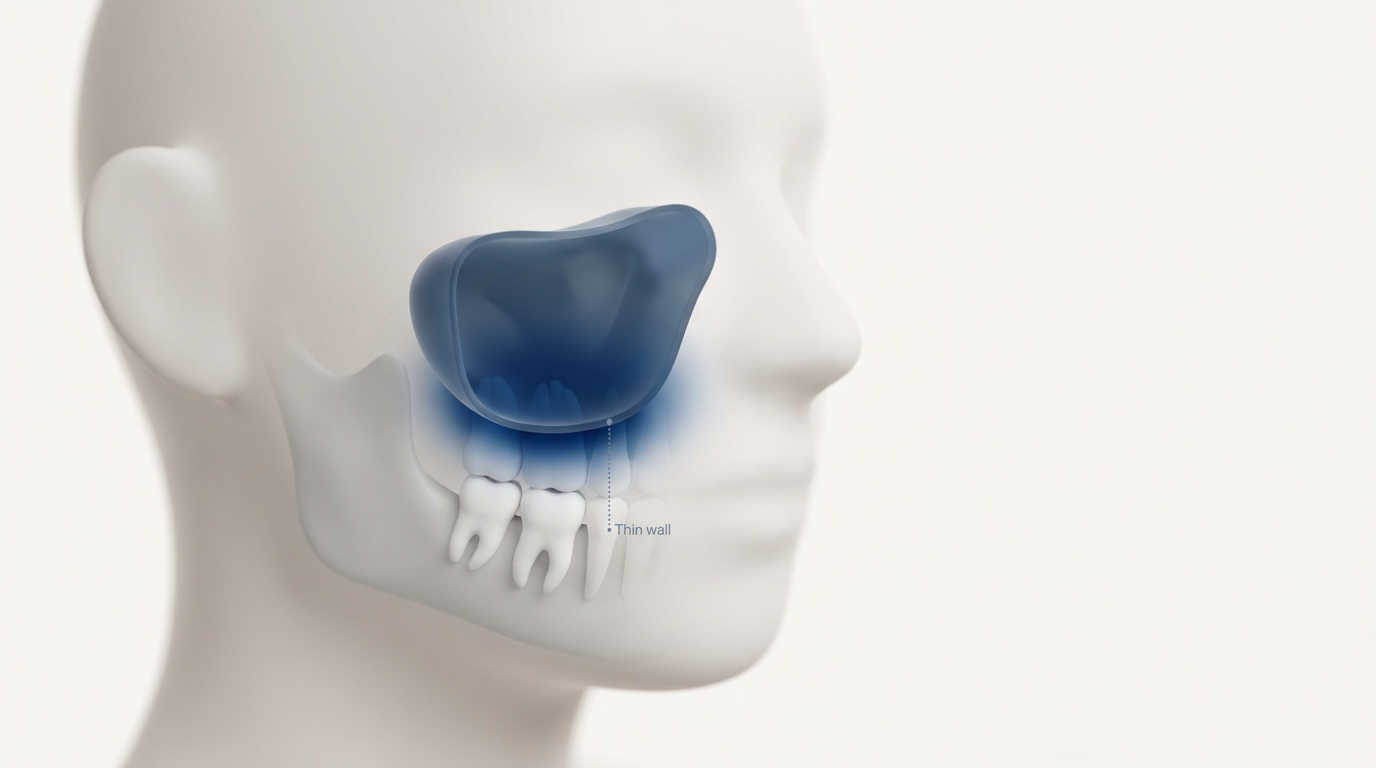
Internal Nasal Valve (INV): The internal nasal valve is typically the narrowest part of the nasal airway and a major determinant of airflow resistance. [1,2] It’s often located about 1.3 cm inside the nostril. [1] In some studies, the internal nasal valve angle is described as roughly 10–15°. [1] When the INV is too narrow—or becomes narrower after trauma or surgery—patients may feel obstructed even if the septum looks not that bad. Many people report, “My breathing never felt the same after I broke my nose,” or “I’m still blocked even after my septum surgery,” which often prompts a closer look at the valve region. [2,4]
External Nasal Valve (ENV): The external nasal valve involves the nostril rim and lower nasal sidewall support. This area may collapse most noticeably during deep inhalation, exercise, or sniffing—when airflow demand is high. Some patients can feel (or see) the nostril sidewall suck in on the worse side.
INV vs ENV collapse—why it changes treatment:
- INV issues often need widening/support near the middle vault (for example, spreader grafts). [2,4]
- ENV issues often need added support to the nostril rim/alar sidewall (for example, alar batten grafts or alar rim grafts). [2,4]
Bottom line: identifying whether the INV or ENV is the bottleneck helps match you to the right treatment.
Symptoms of Nasal Valve Collapse
Common symptoms patients notice:
- Ongoing nasal obstruction (sometimes worse on one side)
- Feeling like you can’t get enough air through your nose
- Worse breathing during exercise, sleep, or deep breaths
- Symptoms that improve when you pull the cheek or side of the nose outward—a classic clue used in clinic-based maneuvers [2,3]
A practical example: if you find yourself gently pulling your cheek sideways while trying to fall asleep—or you notice you breathe better when you hold the side of your nose open—that manual support pattern is often a helpful diagnostic clue to discuss with an ENT. [2,3]
Signs you may see in the mirror:
- The sidewall pinches inward when inhaling
- The nostril rim collapses during a deep breath
How nasal valve collapse can affect sleep and CPAP comfort: Restricted nasal airflow may contribute to mouth breathing, dry mouth, and fragmented sleep in some people. It can also make nasal CPAP harder to tolerate—especially if you feel you’re fighting for air through the nose. For more details, see: Nasal valve collapse and CPAP issues (https://sleepandsinuscenters.com/blog/nasal-valve-collapse-cpap-issues-ent-solutions).
If your breathing improves when you hold your nostril open, mention that to your ENT—it’s a useful clinical clue.
Causes and Risk Factors
Structural or age-related causes: Some people naturally have narrower valve anatomy. In addition, cartilage and soft-tissue support can weaken with aging, increasing the chance of inward collapse during inhalation.
After trauma or prior nasal surgery: A broken nose, facial injury, or scarring can change support structures. Prior nasal surgery may also reduce support or narrow critical angles in ways that contribute to internal or external valve collapse. [4] Subtle framework changes can matter more than they look. [2,4]
Inflammation can stack on top of valve narrowing: Swelling from allergic/nonallergic rhinitis or turbinate enlargement can further narrow an already tight valve region. Treating inflammation may help symptoms—but inflammation control alone typically won’t rebuild structural support if the valve is weak. [2]
Structure sets the baseline; inflammation often stacks on top.

How ENTs Diagnose Nasal Valve Collapse
Diagnosis is primarily based on history and physical exam, often supported by endoscopy and targeted maneuvers. [2]
History: questions your ENT may ask:
- When obstruction is worst (night, exercise, seasonal patterns)
- Prior nasal trauma or surgery
- Whether manually supporting the cheek/nostril improves airflow
Bring specifics if you can: “I’m okay during the day, but blocked when I lie down,” or “My right nostril collapses with a deep breath.” These details help guide a focused exam. [2,3]
Physical exam: what clinicians look for:
- Sidewall or nostril collapse during inspiration
- Asymmetry or prior surgery changes
- Areas that look narrow even before you inhale
The Cottle and modified Cottle maneuvers: These simple in-office maneuvers can help suggest whether valve narrowing is contributing—and may also help distinguish INV vs ENV involvement. [2,3] A clinician may say, “If supporting this area opens your breathing, it suggests your symptoms are coming from the valve region.” The response is supportive—not definitive—evidence in the full clinical picture. [2,3]
Nasal endoscopy: Endoscopy helps assess internal anatomy and rule out other contributors like polyps or severe turbinate enlargement. [2]
Objective airflow tests (when needed): Some clinics use measures like PNIF (Peak Nasal Inspiratory Flow) or rhinomanometry to support evaluation. These tools can add information but don’t perfectly predict which procedure is best for every person. [2]
Careful history, exam, and selective testing help pinpoint whether the valve is your main bottleneck.

Treatment Options (from least to most invasive)
Many care plans take a step-up approach: reduce swelling, try external/internal supports, then consider procedures aimed at adding stable structure.
Address contributing inflammation (may help but won’t fix a weak valve): Treating inflammation can reduce swelling that worsens narrowing. Common approaches include saline irrigation and clinician-guided rhinitis/allergy management. Avoid overusing topical decongestant sprays due to rebound congestion risk. If your obstruction fluctuates (better after a shower, worse in certain seasons, worse around irritants), controlling inflammation may make the baseline valve narrowing feel less severe—even if it doesn’t fully solve the underlying structural issue. [2]
Non-surgical supports you can try: Temporary supports can be helpful for symptoms—and also provide a clue that structural support procedures may work.
- External nasal strips
- Internal nasal dilators (disposable or reusable)
For a practical comparison, see Nasal strips vs internal nasal dilators (https://sleepandsinuscenters.com/blog/nasal-strips-vs-internal-dilators-which-is-best-for-better-breathing).
Start simple: manage swelling and try supports; if relief is incomplete, ask about structural options.

Office-Based / Minimally Invasive Procedures
Many office-based treatments are performed without general anesthesia and may have quicker recovery. Evidence is still evolving, and results depend on anatomy and technique. [2]
Bioabsorbable nasal implants (e.g., Latera): A bioabsorbable implant is designed to support the lateral wall to reduce collapse. Studies report symptom improvement in selected patients. [2] Reported considerations include pain, infection/abscess, and extrusion, as well as variable long-term durability. [2]
Temperature-controlled radiofrequency remodeling (e.g., VivAer radiofrequency): This technique aims to remodel/stiffen tissue to improve airflow. Symptom improvement has been reported in appropriately selected patients, with outcomes that may depend on anatomy and technique. [2]
Who may be a good candidate for office-based options?
- Mild-to-moderate collapse
- A desire to avoid operating-room procedures or who aren’t ideal candidates for them
- Relief with manual support maneuvers (often suggesting a valve component) [2,3]
For the right anatomy, office procedures can help, but expectations should be individualized.
Surgical Treatments (Most Durable for Many Patients)
When nasal valve obstruction is primarily structural, reconstructive approaches are often the most durable option. These procedures are commonly discussed under the umbrella of functional rhinoplasty—surgery focused on breathing and support rather than cosmetic change. [2,4]
Internal Nasal Valve repair: spreader grafts. For INV narrowing, spreader grafts (or autospreader flaps) are widely used to widen/support the internal valve area and improve airflow. [2,4] Surgeons often describe this as rebuilding the frame in the narrowest region so the airway doesn’t pinch inward when you inhale. The exact approach depends on your anatomy and any prior injury or surgery. [2,4]
External Nasal Valve repair: batten grafts and alar rim grafts. For external collapse:
- Alar batten grafts help reinforce weak sidewalls. [2,4]
- Alar rim grafts help support the nostril margin to prevent rim collapse. [2,4]
Why septoplasty/turbinate reduction alone may not solve it: Septum and turbinate procedures can be very helpful when those structures are the main issue. But if nasal valve dysfunction is the key bottleneck, correcting only the septum/turbinates may leave the main problem unchanged—one reason some patients still feel obstructed after otherwise successful septal surgery. [2]
Expected outcomes and what to know: Across studies, reported improvement rates vary widely, and outcomes depend heavily on the procedure, patient selection, and study design. [2] The most meaningful takeaway is that results are highly individualized—especially based on whether the problem is INV vs ENV collapse and whether inflammation or other anatomic factors are also present.
Risks and recovery (high-level): Recovery experiences vary by procedure. In general, people may notice early swelling and congestion, and some procedures can involve bruising. Follow-up is important to monitor healing and long-term airflow stability.
Structural problems often need structural solutions; matching the operation to the anatomy is key.
Lifestyle Tips to Breathe Easier (and Support Treatment)
These strategies don’t replace structural support when it’s needed, but they may reduce symptom spikes.
Sleep-position and nighttime strategies: If nasal breathing feels worse at night, slight head elevation and appropriate humidification may help comfort. If you’re using CPAP or trying to reduce mouth breathing, these comfort-focused adjustments can be a useful baseline while you pursue a structural evaluation.
Reduce inflammation triggers: When symptoms suggest rhinitis, identifying triggers (like smoke or strong fragrances) and addressing allergies can reduce swelling that stacks on top of a narrow valve region.
When to seek evaluation: If obstruction is persistent, worse with deep breathing/exercise, or improves when you pull the cheek/nasal sidewall outward, it may be worth asking specifically about nasal valve obstruction (NVO) during an ENT evaluation. [2,3]
Small daily adjustments can help, but lasting relief usually comes from addressing the true bottleneck.
FAQs About Nasal Valve Collapse
How do I know if it’s nasal valve collapse or a deviated septum? Many people have both. Valve-related problems often cause dynamic narrowing (worse on inhalation) and may improve with support maneuvers like the modified Cottle. [2,3]
Can nasal valve collapse go away on its own? Structural collapse typically doesn’t fully resolve without added support, though symptoms can fluctuate as inflammation changes. [2]
Are implants or radiofrequency as effective as surgery? They can help selected patients and are less invasive, but long-term durability and complication profiles are still being clarified compared with established reconstructive surgery. [2]
Is nasal endoscopy necessary? It’s often helpful to confirm internal anatomy and rule out other causes, though diagnosis still depends heavily on history and physical exam. [2]
Will insurance cover treatment? Coverage varies by plan and by whether the procedure is considered functional (medically necessary) versus cosmetic. It’s reasonable to verify benefits with your insurer.
A focused evaluation helps clarify whether your symptoms stem mainly from the valve, the septum, inflammation, or a mix.
Key Takeaways (Quick Summary)
- The internal nasal valve is a major determinant of airflow resistance and a commonly under-recognized cause of nasal obstruction. [1,2]
- Diagnosis often includes history, exam, endoscopy, and maneuvers like the modified Cottle; objective tests can help in select cases. [2,3]
- For many patients, durable correction involves structural support (spreader grafts for INV; batten/alar rim grafts for ENV). [2,4]
- Office-based options (bioabsorbable implants, radiofrequency remodeling) may help selected patients; evidence is evolving and outcomes vary by anatomy and technique. [2]
Think bottleneck: once you identify where the airflow pinches, treatment choices become clearer.
Book an appointment
If you suspect nasal valve obstruction—or you’re still congested after treatment for a septum, turbinates, or allergies—an ENT evaluation can clarify whether the valve is the main bottleneck and what options fit your anatomy. To schedule a visit with Sleep and Sinus Centers of Georgia, book here: https://www.sleepandsinuscenters.com/
Medical disclaimer
This article is for general education and does not provide medical advice, diagnosis, or treatment. Nasal obstruction has multiple possible causes, and the right evaluation and treatment depend on your anatomy, symptoms, and medical history. For personal guidance, consult a qualified clinician.
Sources
1. Liu DH. Anatomy and Physiology of the Nasal Valves. 2025. https://pubmed.ncbi.nlm.nih.gov/39426874/
2. Pirola F. Nasal valve obstruction: a comprehensive analysis and management algorithm. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11983596/
3. Internal vs External Nasal Valve Collapse. 2024. https://www.backtable.com/shows/ent/articles/nasal-valve-collapse-internal-vs-external
4. Medscape. Internal Valve Stenosis / Rhinoplasty overview. 2022. https://emedicine.medscape.com/article/877468-overview
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.