
Nasal Blockage and Sleep Apnea: Causes, Symptoms, and Treatment Options
Introduction — Why Your Nose Matters in Sleep Apnea
Obstructive sleep apnea (OSA) happens when the upper airway repeatedly narrows or collapses during sleep, leading to breathing interruptions, oxygen drops, and frequent microarousals. While OSA is usually driven by collapse in the throat (not the nose), your nose still plays a major role in how well you sleep—and how comfortable OSA treatment feels.
Here’s the key takeaway: nasal blockage can worsen sleep quality and make CPAP harder to use, but treating nasal obstruction often does not significantly change OSA severity (AHI) for most people. However, improving nasal airflow—sometimes including nasal surgery—may help selected patients, particularly by improving comfort and CPAP tolerance rather than curing OSA. Evidence from systematic reviews and clinical studies supports this overall pattern. [1–4]
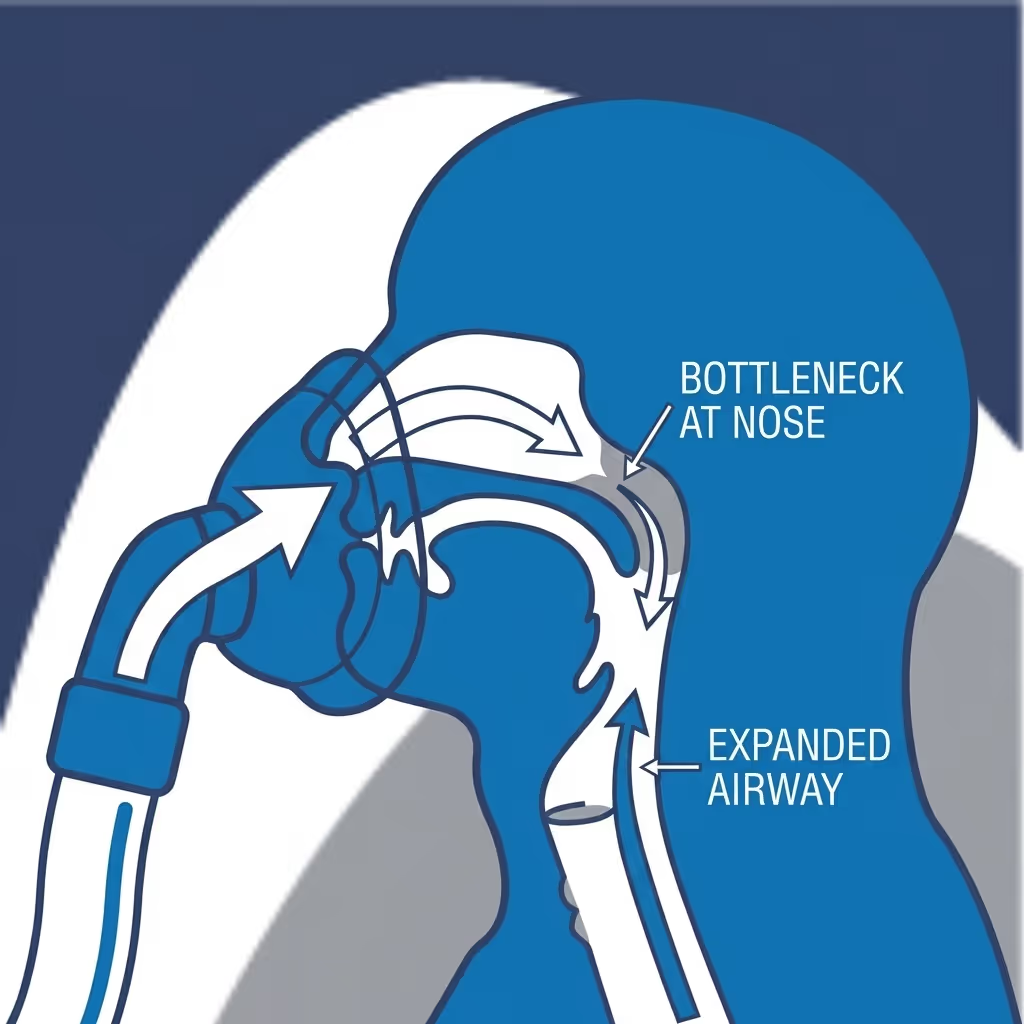
A practical way to think about it: the nose is rarely the “main collapse point” in OSA, but it can be the bottleneck that determines how easy (or miserable) breathing and CPAP feel at night.
If you want more background on why the nose supports better sleep, see our post on nasal breathing benefits for better sleep quality: https://sleepandsinuscenters.com/blog/nasal-breathing-benefits-for-better-sleep-quality
Quick Definitions (So the Rest Makes Sense)
What is nasal blockage (nasal obstruction)?
Nasal obstruction is the sensation of reduced airflow through one or both nostrils. It can be constant (all day, every day) or fluctuate due to the normal “nasal cycle,” where each side alternates being more open.
Some people notice this most at night: they fall asleep “fine,” then wake up feeling like one side is sealed shut. That pattern can still be normal—but persistent, severe, or one-sided obstruction deserves a closer look.
What is obstructive sleep apnea (OSA)?
OSA is a sleep-related breathing disorder where the airway repeatedly collapses during sleep. Severity is often described using:
- AHI (Apnea-Hypopnea Index): number of apnea/hypopnea events per hour of sleep (a measure of breathing-event frequency, not a direct measure of symptom severity)
For a practical guide, read our overview: https://sleepandsinuscenters.com/blog/ahi-score-explained-understanding-your-sleep-apnea-severity
What is CPAP and why does nasal airflow affect it?
CPAP (continuous positive airway pressure) keeps the airway open by delivering pressurized air through a mask. When the nose is blocked, resistance rises and CPAP can feel uncomfortable—often leading to mouth breathing, mask leaks, dryness, and frustration. That’s why nasal congestion affecting CPAP tolerance is such a common barrier to successful treatment.
A simple analogy: CPAP works best when air can flow through a “clear hallway.” If the hallway is narrowed (swollen turbinates, a deviated septum, congestion), the same airflow can feel more forceful and harder to tolerate—like trying to breathe through a pinched straw.

The Connection — Does Nasal Blockage Cause Sleep Apnea?
This is where the nuance matters. Nasal blockage and sleep apnea often show up together, but that doesn’t always mean one directly causes the other.
- Nasal obstruction can contribute to snoring, mouth breathing, and sleep disruption.
- OSA, however, is most often driven by throat-level collapse (soft palate, tongue base, and surrounding tissues).
Research suggests that treating nasal obstruction (with medication or surgery) does not consistently reduce AHI for most people with OSA. [1] In other words: improving the nose often improves the experience of sleep, but not always the headline number on the sleep study.
How nasal blockage can worsen sleep (even if AHI doesn’t change much)
- awakenings/arousals and “lighter” sleep
- snoring intensity and bed-partner disturbance
- daytime sleepiness and quality-of-life impacts
This is one reason people with “stuffy nose sleep apnea” complaints can feel better after addressing the nose—even if a sleep study number doesn’t move much. [1]
Clinician-style summary you’ll often hear: We’re not promising the nose fix will cure apnea—but we are trying to make sleep and CPAP more tolerable.

Symptoms to Watch For
Nasal blockage symptoms (day and night)
Common nasal obstruction symptoms include:
- chronic congestion (or congestion that switches sides)
- postnasal drip or throat clearing
- reduced sense of smell
- facial pressure (more common when sinus inflammation is involved)
- needing to breathe through the mouth at night
A concrete example: if you routinely wake with a dry mouth and find your jaw dropped open, nasal blockage (or fluctuating congestion) may be nudging you into mouth breathing—even if you don’t feel “congested” during the day.
Sleep apnea symptoms that can overlap—or worsen with nasal obstruction
Symptoms commonly reported in OSA include:
- loud snoring
- choking/gasping sounds during sleep
- restless, fragmented sleep
- morning headaches
- dry mouth on waking
- daytime fatigue or sleepiness
CPAP-specific signs that the nose may be a major barrier:
- removing the mask at night without meaning to
- difficulty tolerating pressure
- high leak (especially with mouth breathing)
- feeling “air hunger” through a congested nose
If CPAP feels okay on some nights but impossible on others, fluctuating nasal inflammation (allergies, irritants, infections) is a common—and very fixable—piece of the puzzle.
When symptoms are urgent (seek care)
Educationally, it’s helpful to know red flags that typically warrant prompt medical evaluation, such as significant nosebleeds, severe facial swelling, high fever, vision changes, or severe sleepiness that affects driving safety. Chest pain or concerning cardiovascular symptoms should be evaluated urgently.
Common Causes of Nasal Blockage (And How Each Affects Sleep)
Inflammatory causes
- Allergic rhinitis (seasonal/perennial): A leading cause of nighttime congestion. Learn more: https://sleepandsinuscenters.com/blog/chronic-allergic-rhinitis-and-its-impact-on-sleep-quality
- Nonallergic rhinitis: Triggered by irritants, weather/temperature shifts, strong odors, or smoke.
Inflammation can swell nasal tissues, increasing resistance—often felt most when lying down. That’s one reason someone might say, “I breathe fine all day, but the second I’m in bed, my nose closes up.”
Structural causes
- Deviated septum: A common structural reason for one-sided or persistent blockage. If you’re exploring the link between deviated septum concerns and CPAP comfort, this page is a helpful starting point: https://sleepandsinuscenters.com/deviated-septum-relief
- Turbinate hypertrophy: Enlarged turbinates can narrow airflow; questions about turbinate reduction and sleep apnea often come up when CPAP feels intolerable.
- Nasal valve collapse: Weakness or narrowing at the nasal entrance can dramatically reduce airflow, especially on deep breaths.
- Adenoid hypertrophy: More common in children.
A useful self-observation (not a diagnosis): if pulling your cheek gently to the side improves airflow, the nasal valve area may be contributing.
Sinus-related causes
- Chronic sinusitis (inflammation): Swelling can reduce airflow and worsen night congestion.
- Nasal polyps: Soft growths that can significantly block airflow.
Medication-related causes
- Rebound congestion from frequent use of topical decongestant sprays (like oxymetazoline). If this sounds familiar, read: https://sleepandsinuscenters.com/blog/afrin-rebound-how-long-does-nasal-congestion-last-after-use
A common story: a spray helps for a night or two, then it “stops working,” and suddenly it feels impossible to sleep without it. That cycle is exactly what rebound congestion can look like.
How Doctors Evaluate Nasal Blockage in People With Suspected/Confirmed OSA
History and symptom patterns
Evaluation often starts with patterns such as:
- day vs. night congestion
- one nostril vs. both
- seasonal triggers, pets, dust exposure, workplace irritants
- whether nasal obstruction is the main reason CPAP isn’t working
In other words, clinicians often try to determine if the relationship is primarily nasal obstruction and sleep apnea occurring together—or nasal obstruction actively limiting therapy success.
Physical exam + nasal endoscopy (when needed)
An exam may assess the septum, turbinates, nasal valve area, and the presence of polyps or significant inflammation. Endoscopy can provide a more detailed view when symptoms and exam don’t fully match.
Sleep testing to assess OSA severity
Sleep testing (home or in-lab) is important because nasal symptoms alone can’t define OSA severity. It also helps prevent the common misconception that fixing the nose automatically “fixes” sleep apnea. [1]

Treatment Options (Patient-Friendly, Step-by-Step)
Treating nasal obstruction medically (often first-line)
Common non-surgical treatment categories include:
- saline rinses/sprays to clear mucus and irritants
- intranasal corticosteroid sprays to reduce inflammation (technique and consistency matter)
- antihistamines when allergies are a clear driver
- anticholinergic sprays for prominent runny-nose patterns
- allergy evaluation and targeted treatment when appropriate: https://sleepandsinuscenters.com/allergy-testing
Realistic expectations: Many patients notice better breathing comfort, reduced snoring, and improved sleep quality, but AHI improvement is inconsistent across studies. [1] This is why treating nasal blockage and sleep apnea often focuses on symptoms and treatment tolerance—not just the AHI number.
A helpful mindset: medical therapy is often about making the nose less reactive and less swollen over time, not “instantly opening” it for one night.

CPAP Tips When Nasal Blockage is the Barrier
Equipment adjustments that can help right away
- heated humidification to reduce dryness and irritation
- mask refitting (nasal pillows, nasal mask, or full-face options)
- addressing mouth breathing and leaks
If mask choice is the big question, compare options here: https://sleepandsinuscenters.com/blog/full-face-vs-nasal-pillow-masks-which-cpap-mask-is-best-for-you
For congestion-specific troubleshooting, see: https://sleepandsinuscenters.com/blog/blocked-nose-during-cpap-ent-strategies
One practical example: someone who does great with nasal pillows in the spring may need a different approach during fall allergy season—or may do better once inflammation is treated consistently.
Practical bedtime strategies
- saline rinse before bed (when appropriate)
- bedroom allergen control (washing bedding, reducing dust, HEPA filtration)
- avoiding overuse of topical decongestant sprays (to reduce rebound risk)
Small changes add up. When nasal resistance drops even a little, CPAP often feels “less pushy,” and leaks become easier to control.

When Nasal Surgery May Help (Especially for CPAP Users)
The evidence in plain language
Across research, nasal surgery usually does not significantly change AHI for most OSA patients. [1] Where surgery can matter most is comfort and treatment delivery—especially when nasal blockage and sleep apnea collide through CPAP intolerance.
In selected patients, studies suggest nasal surgery may:
- lower required CPAP pressures by about 2.66 cm H2O on average in the cited review [2]
- improve adherence to CPAP after nasal surgery; some studies reported increases in average nightly use, for example from about 3.0 to 5.5 hours/night in specific cohorts [2–4]
That pressure change may sound small, but for some patients it’s the difference between “I can’t stand this” and “I can finally sleep with it.”
Types of procedures commonly considered
- septoplasty (for septal deviation)
- turbinate reduction
- nasal valve repair
- polyp removal or sinus procedures when inflammatory obstruction is significant
Who benefits most (patient selection is key)
- nasal obstruction is clearly the primary barrier to CPAP success
- other barriers (mask fit issues, untreated insomnia, inadequate support/education) are also addressed
It’s also worth noting that research is heterogeneous—different nasal problems, different procedures, and different outcomes—so results don’t apply equally to everyone. [1–2]
What to expect after surgery (realistic outcomes)
- improved nasal airflow and comfort
- easier CPAP tolerance (and sometimes lower pressure needs)
- better consistency using CPAP
But many will still need CPAP or another OSA therapy after nasal surgery, depending on airway anatomy and baseline OSA severity. [1]
A realistic patient-style quote: “Surgery didn’t ‘erase’ my sleep apnea, but it made CPAP feel doable—and that changed everything.”
Other OSA Treatments (If Nasal Obstruction Isn’t the Whole Story)
If the main issue isn’t the nose—or if OSA remains significant—other options may include oral appliance therapy for selected patients, weight management and positional strategies when appropriate, other upper-airway procedures, or hypoglossal nerve stimulation for carefully selected candidates.
Lifestyle Tips to Reduce Nighttime Nasal Blockage
Bedroom environment
- reduce allergens (dust-mite covers, hot-water bedding wash)
- aim for comfortable humidity (too dry can irritate; too humid can encourage mold)
Daily habits
- track triggers (pollen, pets, irritants)
- avoid smoking/vaping exposure
- maintain hydration
Medication safety reminders
Topical decongestant sprays are generally intended for short-term use; frequent use can contribute to rebound congestion.
FAQs
Can nasal blockage cause sleep apnea?
Nasal obstruction can worsen snoring and sleep disruption, but OSA is usually driven by throat collapse. Nasal treatment alone rarely normalizes AHI. [1]
Will fixing a deviated septum cure my sleep apnea?
A deviated septum procedure often improves airflow and can make CPAP easier, but it typically doesn’t “cure” OSA on its own. Follow-up testing helps clarify what changed. [1]
Can nasal surgery reduce my CPAP pressure?
In selected patients, studies show nasal surgery can reduce therapeutic CPAP pressures by about 2–3 cm H2O on average in some studies. [2]
If my AHI doesn’t improve, why do I feel better after nasal treatment?
Because sleep quality can improve through fewer arousals, less snoring, and better comfort—even without a major AHI change. [1]
What’s the best CPAP mask if my nose is blocked?
It depends on how reliable nasal breathing is and what’s driving the blockage. A full-face mask can help when nasal breathing is inconsistent, but addressing nasal obstruction may allow a more comfortable nasal interface.
Conclusion + Next Steps
Nasal blockage and sleep apnea are closely linked in day-to-day life: nasal obstruction can fragment sleep and make CPAP feel harder than it should. Treating nasal blockage—medically and, in selected cases, surgically—can be valuable for improving sleep quality and making CPAP more tolerable. However, nasal treatment alone is not a guaranteed way to reduce AHI.
If nasal obstruction is your #1 CPAP barrier, an evaluation can help identify the cause and map out options. If you think you may benefit from evaluation, consider scheduling an appointment with a qualified clinician: https://sleepandsinuscenters.com/appointments
Citations
1. Nasal Obstruction and Obstructive Sleep Apnea: A Systematic Review (2022). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9449074/
2. The effect of nasal surgery on CPAP adherence… systematic review and meta-analysis (2015). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4288609/
3. Nasal surgery improves PAP compliance… (2023). Scientific Reports (Nature). https://www.nature.com/articles/s41598-023-31588-7
4. In patients with OSA and nasal obstruction does nasal surgery improve CPAP compliance? (2024). LWW Evidence-Based Practice. https://journals.lww.com/ebp/fulltext/2024/06000/in_patients_with_obstructive_sleep_apnea__osa__and.15.aspx
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.






