Nasal Airway Obstruction: Causes, Symptoms, and Treatment Options
Overview—What “nasal airway obstruction” means (and why it matters)
Nasal airway obstruction means having difficulty moving air through one or both sides of your nose. Some people notice it as “stuffiness,” while others describe it as not getting enough airflow—even when they don’t feel “sick.” A common experience is: “I can breathe through my mouth fine, but my nose just doesn’t move air the way it should.”
It matters for more than comfort. Ongoing blockage can affect sleep quality, snoring, exercise tolerance, and even how well someone can use CPAP for sleep apnea. Importantly, obstruction isn’t always “just congestion.” Many cases are structural, inflammatory, or a combination—so treatment is usually individualized rather than one-size-fits-all. Position statements and reviews emphasize the wide variety of underlying causes and the need to tailor evaluation and management to the patient. [2][3]
Nasal anatomy in plain English (quick guide)
A few key structures help explain why small changes can create big symptoms—especially because the nasal airway has natural “pinch points”:
- Septum: the “wall” that divides the nose into right and left sides.
- Turbinates: structures along the sidewalls that filter, warm, and humidify air.
- Nasal valves: the narrowest part of the nasal airway (near the front of the nose). Because they’re a natural bottleneck, even mild narrowing or weakness here can significantly reduce airflow—like a slight squeeze in a drinking straw that suddenly makes it hard to sip.
In short: nasal obstruction is common, often multifactorial, and best managed with a tailored plan.

Common causes of nasal airway obstruction
A simple way to frame causes is: blocked by swelling, blocked by structure, or blocked by both. In real life, many patients have more than one contributor, which is why an ENT visit often focuses on finding the “main bottleneck(s).”

Structural causes (the “plumbing” issues)
Deviated septum
A deviated septum occurs when the septum is off-center or has spurs that narrow one side of the nose. Some people feel obstruction all the time; others notice it more at night or when lying down. It can also feel “alternating” if the more open side changes with normal nasal cycling.
Septal deviation commonly coexists with turbinate enlargement and/or valve problems, which is why evaluation usually looks beyond the septum alone rather than assuming one finding explains everything.
Learn more about deviated septum treatment options: https://sleepandsinuscenters.com/deviated-septum-relief
Turbinate hypertrophy (enlarged turbinates)
Turbinate hypertrophy means the turbinates are enlarged—often due to allergies or chronic irritation. Sometimes swelling is mainly “soft tissue” and improves with consistent medical therapy (especially daily nasal steroid spray with correct technique). In other cases, enlargement can be more persistent and may benefit from a procedure designed to reduce turbinate size while preserving function.
A helpful way to picture it: turbinates are “air-conditioning fins” for your nose. They’re supposed to be there. The goal is not to remove them, but to restore enough space for airflow while keeping their warming and humidifying role.
Deeper overview of turbinate reduction: https://sleepandsinuscenters.com/blog/everything-you-need-to-know-about-turbinate-reduction
Nasal valve collapse (internal or external valve)
Nasal valve collapse is often described as “sidewall weakness” near the nostril where the tissue narrows or collapses inward during breathing—especially with deep inspiration or exercise. Some people notice it most when walking briskly, climbing stairs, or during workouts, when the demand for airflow increases.
It can be under-recognized, and diagnostic approaches vary across clinicians. Reviews note there is no single standardized, universally accepted diagnostic test, so ENTs often combine history, exam findings, and supportive testing. [1] Clinically, a patient might say, “I feel like the side of my nose caves in when I breathe in.”
More detail on nasal valve collapse treatments: https://sleepandsinuscenters.com/blog/nasal-valve-collapse-treatment-effective-solutions-and-options

Other structural causes to mention briefly
- Nasal polyps or other growths
- Scar tissue (synechiae) after trauma or prior nasal surgery
- Rare but important: tumors—often considered when symptoms are one-sided and progressively worsening
Inflammatory causes (the “swelling” issues)
Allergic rhinitis: Can be seasonal or year-round. Many people notice patterns—pollen seasons, dust exposure, pets—and may have associated sneezing, itching, or watery eyes. Symptoms often improve with consistent therapy rather than “as-needed” use.
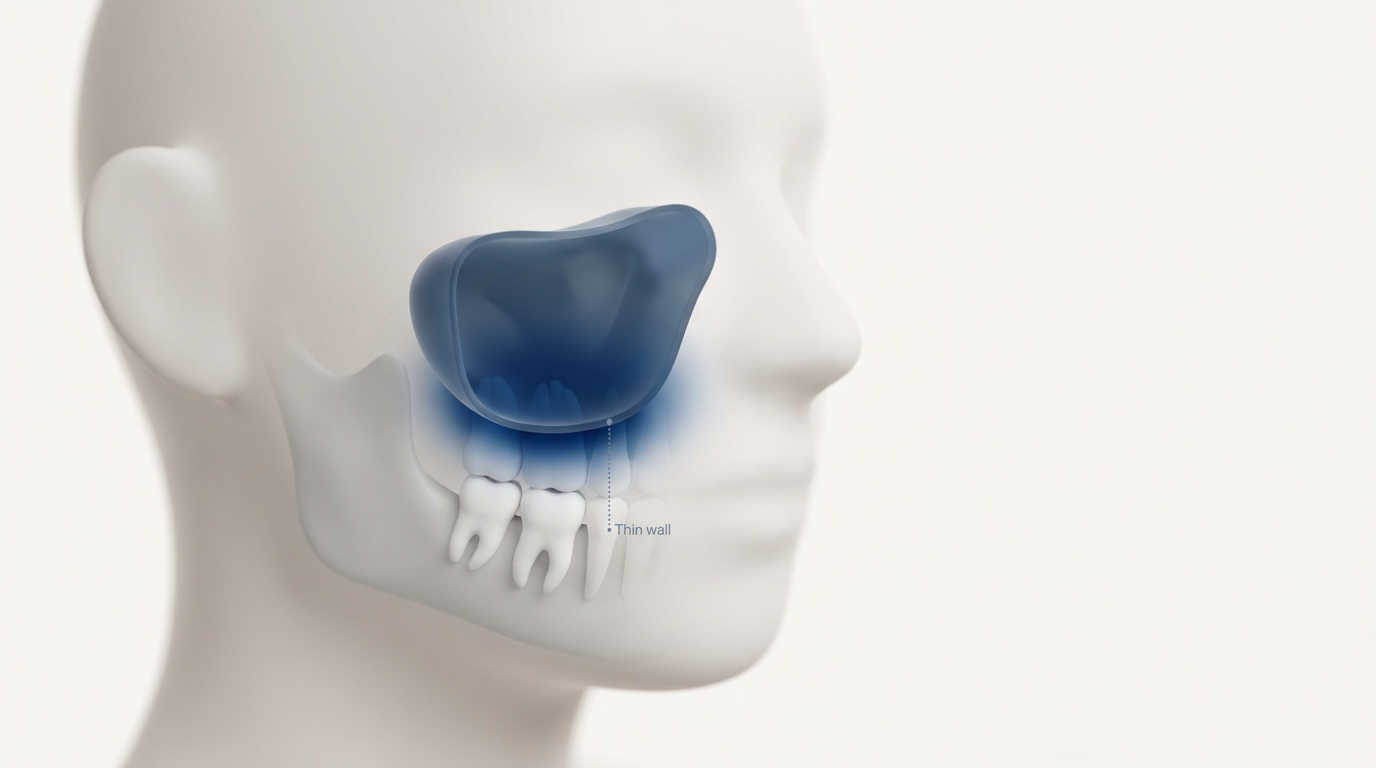
Non-allergic rhinitis / chronic rhinitis: Not all chronic nasal symptoms are allergy-driven. Irritants (smoke, fragrances), weather/temperature changes, and other triggers may cause ongoing inflammation and swelling. Some patients describe sudden congestion in cold air or when entering strongly scented environments.
Acute colds, sinus infections, chronic sinusitis: A cold or infection can temporarily swell the nasal lining and narrow airflow. Chronic sinusitis or recurring infections may contribute to longer-term symptoms and fluctuations, especially when congestion is paired with facial pressure, drainage, or smell changes.
Medication-related causes
Rebound congestion from decongestant sprays (rhinitis medicamentosa): Topical decongestant sprays can provide short-term relief, but using them longer than directed can lead to rebound congestion—where stopping the spray makes blockage feel worse. This can create a frustrating cycle: brief relief followed by worsening obstruction, prompting more frequent use.
Bottom line: many people have a mix of swelling and structural issues, so pinpointing the main contributors is key.
Symptoms—how nasal airway obstruction can show up day and night
Classic symptoms
- Stuffy nose (one side or both)
- Trouble breathing through the nose during exercise
- Mouth breathing; dry mouth or sore throat in the morning
- Sometimes reduced sense of smell
Sleep-related symptoms (high patient interest)
Nasal airway obstruction often feels worse when lying down. Some people notice:
- Snoring or noisy breathing at night
- Restless sleep or waking unrefreshed
- Difficulty tolerating CPAP due to nasal blockage
A practical example: a patient may be able to fall asleep, but wake up repeatedly because nasal breathing becomes harder as congestion and swelling increase overnight.

A quick “pattern” clue (not a diagnosis)
Many people find these patterns helpful to mention to their clinician:
- Mostly one-sided and persistent: raises suspicion for structural narrowing (like septal deviation or valve issues).
- Fluctuates with seasons/irritants: suggests an inflammatory driver (like allergic or non-allergic rhinitis).
- Worse with deep breaths or exercise: can point toward nasal valve collapse.
Overlap is common, so patterns are clues—not final answers.
When to seek care urgently (red flags)
Educationally, these symptoms are commonly treated as “red flags” to discuss promptly with a clinician:
- Persistent one-sided obstruction should be evaluated promptly, because it can have structural or, less commonly, more serious causes.
- Frequent nosebleeds, facial swelling, severe pain, or vision changes
- Symptoms that continue to worsen despite reasonable treatment efforts
In short, track your symptom patterns and seek prompt evaluation for one-sided or worsening problems.
How ENTs diagnose nasal airway obstruction (and why it can be tricky)
The diagnostic challenge (no single “gold standard”)
There isn’t one definitive test that identifies every cause of nasal airway obstruction. Many causes overlap, and different blockage patterns can feel similar to patients. Reviews and position statements highlight heterogeneity in both diagnosis and treatment—especially for nasal valve problems—so ENTs typically combine history, exam, and selective testing. [1][2][3]
History questions your clinician may ask
- Is it worse on one side or both? Constant or alternating?
- Do you notice triggers (allergies, colds, exercise, lying down)?
- Any prior nasal trauma or surgery?
- How often do you use decongestant sprays?
Small details can matter. For example, “It’s fine sitting up but terrible at night” may lead an ENT to think differently than “It’s always blocked on the left.”
Physical exam and in-office evaluation
Evaluation often includes:
- External inspection (including signs of valve narrowing or collapse)
- Internal nasal exam
- Nasal endoscopy when needed to see deeper structures, inflammation, polyps, or scarring
Endoscopy can be especially useful when symptoms and the front-of-nose exam don’t fully match—helping confirm whether swelling, polyps, or scarring is contributing.
Symptom scoring tools (patient-reported outcomes)
Many ENTs use the NOSE score (Nasal Obstruction Symptom Evaluation). It’s a short questionnaire that quantifies symptom severity and helps track response to treatment over time—essentially turning “How blocked do you feel?” into a measurable number.
It’s widely used in clinical research on nasal obstruction treatments, which helps clinicians compare outcomes across different approaches. [4][5]
Objective airflow tests (when available)
Some clinics use supportive airflow testing such as:
- Peak Nasal Inspiratory Flow (PNIF) test: a simple measure of nasal airflow. In a multicenter randomized trial, PNIF improved after septoplasty compared with continued medical management (reported improvement of +29.3 L/min). [5]
- Acoustic rhinometry or rhinomanometry: specialized measurements that estimate nasal geometry or resistance; availability varies and results are often interpreted alongside clinical findings. [1]
Takeaway: ENTs combine your history, exam, and selective tests (like NOSE and PNIF) to pinpoint the main airflow bottlenecks.
Treatment options (stepwise, patient-friendly)
Because nasal airway obstruction commonly has more than one contributor, many people do best with a stepwise plan that addresses both inflammation and structure when appropriate. Shared decision-making is key, and combination approaches are frequently discussed in the medical literature. [1]
At-home and lifestyle measures (good first steps and good add-ons)
- Saline spray or saline irrigation (with safe water practices and proper technique)
- Humidifier use in dry environments
- Bedroom-focused allergen reduction strategies
- Avoid smoke/vaping and strong irritants
- Use caution with topical decongestant sprays to help prevent rebound congestion
These steps often won’t “fix” a significant structural issue, but they can reduce swelling and make other treatments work better.
Medical treatments (reduce inflammation/swelling)
Depending on symptom patterns and exam findings, options may include:
- Intranasal steroid sprays (best results usually come from consistent daily use and good technique)
- Antihistamines when allergies are a major driver
- Ipratropium nasal spray for prominent runny nose
- Allergy evaluation and immunotherapy when appropriate
Position statements support evaluating and treating contributing conditions as part of a comprehensive plan. [2][3]
In short: start with sound medical therapy and habits, then layer in procedures if a structural bottleneck remains.

Procedural and surgical treatments (when structure is the problem—or part of it)
Septoplasty (straightening the septum)
Septoplasty is designed to correct airflow limitation from a deviated septum. It’s often considered when symptoms correlate with septal deviation on exam, especially when medical therapy doesn’t provide enough relief. Many patients report noticeable improvement after septoplasty, though results vary by individual. In a multicenter randomized trial, septoplasty significantly improved symptom scores (including NOSE and SNOT-22) and improved airflow as measured by PNIF compared with continued medical management. [5]
Turbinate reduction (shrinking enlarged turbinates)
Turbinate reduction aims to decrease turbinate size to improve airflow while preserving the turbinates’ important humidifying and filtering functions. Techniques vary (including submucosal reduction and radiofrequency-based approaches). Turbinate procedures are frequently combined with septoplasty when both septal deviation and turbinate hypertrophy contribute to narrowing.
- Learn more about turbinate reduction: https://sleepandsinuscenters.com/blog/everything-you-need-to-know-about-turbinate-reduction
Nasal valve treatments (addressing sidewall collapse)
Traditional valve surgery / functional rhinoplasty approaches
When the valve area is clearly narrow or collapses, traditional surgical approaches can strengthen or widen the nasal valve region. These may be combined with septoplasty and/or turbinate reduction to address multiple “bottlenecks” in one plan. [1]
Minimally invasive, office-based options (newer technologies)
- Bioabsorbable lateral wall implant (e.g., LATERA implant) — Studies and policy summaries report improved NOSE scores, with low implant retrieval rates in cited materials, though rates vary across studies. [6]
- Radiofrequency remodeling (e.g., VivAer radiofrequency remodeling) — Published studies, including randomized and longer-term data, show clinically meaningful NOSE score improvements in selected patients. [4]
Why combined treatment often works better than “one procedure”
It’s common for septal deviation, turbinate hypertrophy, and nasal valve collapse to coexist. Treating only one area can leave another area as the limiting factor—like widening one lane of traffic when the next intersection still bottlenecks. Reviews emphasize individualized planning and the frequent need to address multiple sites to optimize outcomes. [1]
- More on valve-focused treatments: https://sleepandsinuscenters.com/blog/nasal-valve-collapse-treatment-effective-solutions-and-options
- Septal-focused information: https://sleepandsinuscenters.com/deviated-septum-relief
Recovery expectations (general, not prescriptive)
- The first week: swelling, congestion, and gradually improving airflow
- The following weeks: steadier improvement as swelling resolves
Contacting the surgical team is typically recommended if there is heavy bleeding, fever, severe or worsening pain, or rapidly increasing swelling.
Key point: procedures target structure, and combining techniques can address more than one bottleneck when needed.
How to choose the right treatment plan (shared decision-making)
Matching the treatment to the cause
A practical approach is to identify whether symptoms are:
- Swelling-dominant (more responsive to medications and trigger control)
- Structure-dominant (more likely to benefit from procedures)
- Mixed (often best managed with a combination plan)
Tracking symptoms with tools like the NOSE score can help measure progress, clarify whether a plan is working, and guide next steps. [1][4][5]
Questions to ask at your ENT visit
- Is my obstruction mostly septum, turbinates, valves, inflammation—or a mix?
- Which findings support that conclusion (NOSE score, Peak Nasal Inspiratory Flow test, endoscopy)?
- Would I benefit from combined procedures?
- What alternatives are reasonable if I’m not ready for surgery?
Evidence gaps (transparent, patient-friendly)
While there is supportive evidence for several treatments, there are still gaps—especially fewer long-term, head-to-head comparative studies across all options and continued lack of fully standardized diagnostic algorithms for nasal valve obstruction. [1]
In brief: align treatment to the main cause(s), track results, and adjust the plan collaboratively.
FAQs
How can I tell if it’s allergies or a deviated septum?
Allergies often fluctuate with triggers and tend to improve with consistent medical therapy. A deviated septum is more likely to cause persistent or asymmetric blockage—though overlap is common, and many people have more than one contributor.
What is the NOSE score and why does my ENT use it?
The NOSE score is a validated questionnaire that measures how severe nasal obstruction feels and helps track improvement over time. It’s commonly used in studies evaluating nasal obstruction treatments. [4][5]
Do I need a CT scan for nasal airway obstruction?
Not always. Many cases are diagnosed with history, exam, and sometimes nasal endoscopy, plus symptom scoring. Imaging may be used when sinus disease, polyps, or other concerns are suspected.
Is septoplasty proven to work?
For appropriately selected patients, there is evidence of benefit. A multicenter randomized trial found septoplasty improved NOSE and SNOT-22 scores and increased airflow (PNIF) compared with continued medical management. Individual results vary. [5]
Are office-based nasal valve treatments effective?
Studies report clinically meaningful NOSE improvements for both bioabsorbable implants and radiofrequency remodeling in selected patients, with low implant retrieval rates reported in cited summaries; rates vary by study. [4][6]
Can more than one issue be causing my blockage?
Very often. Deviated septum, turbinate hypertrophy, and nasal valve collapse frequently coexist, and combination treatment can be important for meaningful improvement. [1]
Conclusion + Next Step
Nasal airway obstruction is common—and treatable—but the “best” solution depends on identifying where airflow is being limited (swelling, structure, or both). If symptoms are affecting sleep, exercise, or day-to-day quality of life, an ENT evaluation can clarify the likely causes and outline options ranging from medical therapy to in-office procedures and surgery.
To learn what may be driving your symptoms and review personalized options, book an appointment with Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Sources
1. Review on diagnostic/treatment heterogeneity and lack of a single gold standard: https://pmc.ncbi.nlm.nih.gov/articles/PMC11983596/
2. AAO-HNS Position Statement (2023): https://pmc.ncbi.nlm.nih.gov/articles/PMC12046381/
3. American Rhinologic Society Position Statement (2022): https://pmc.ncbi.nlm.nih.gov/articles/PMC12964075/
4. Stolovitzky et al. (2019), International Forum of Allergy & Rhinology (radiofrequency remodeling outcomes)
5. Carrie et al. (2023), Multicenter Septoplasty Randomized Trial (NOSE/SNOT-22/PNIF improvement)
6. LATERA implant policy summary (retrieval rate and outcomes): https://www.keystonefirstpa.com/content/dam/keystone-first/keystone-first-pa/pdf/provider/resources/clinical/20260114/ccp1441-latera-absorbable-nasal-implant.pdf.coredownload.inline.pdf
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.