

Nasal Valve Explained: The Overlooked Cause of Nasal Obstruction and Blocked Breathing
A “stuffy nose” is often blamed on allergies, a deviated septum, or sinus trouble. But some people keep feeling blocked even after sprays, antihistamines, or a “normal” scan. One commonly missed reason is nasal valve dysfunction—a structural airflow problem that can be subtle on imaging but very noticeable when you breathe.
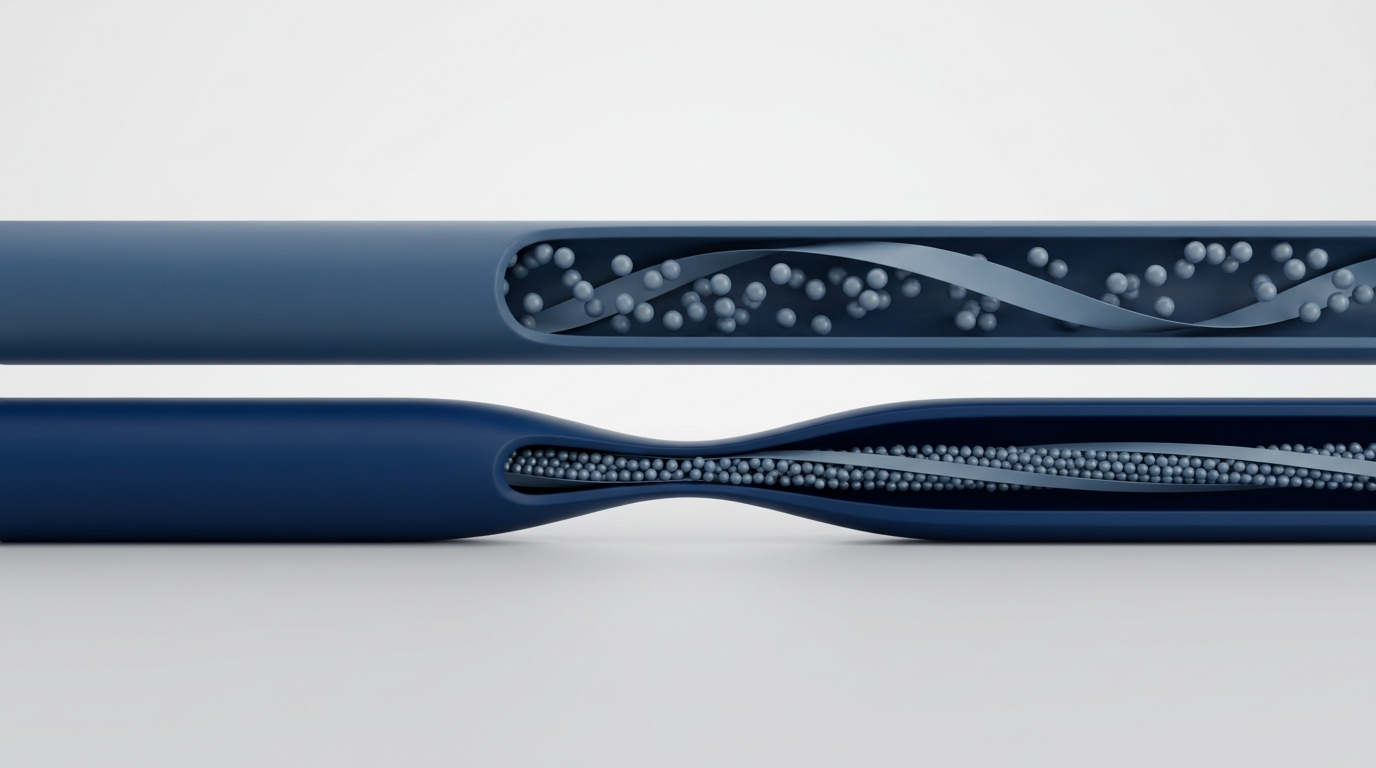
Think of it this way: if you pinch a drinking straw even slightly, the whole sip gets harder. The nasal valve is that pinch point for nasal airflow. Below is a clear, patient-friendly guide to what’s going on, how it’s checked in clinic (including the Cottle maneuver), and what treatments can help—from nasal strips to procedures like a spreader graft or LATERA implant.
Why “Stuffy Nose” Isn’t Always Allergies or a Deviated Septum
The common frustration: congestion with normal scans or failed treatments. Some people try saline, steroid sprays, and allergy meds—maybe even discuss septum surgery—yet still feel they can’t get enough air. You may hear, “Your CT looks fine,” or, “There’s not much mucus.”
Often, the problem isn’t “more congestion.” It’s airflow mechanics. Air has to pass through a narrow, structured segment—and if that segment is too tight or too weak, breathing can feel restricted even when the lining looks relatively calm.
Key point: the nasal valve is the narrowest part of the nasal airway, and small changes there can create a big increase in resistance and the sensation of obstruction.¹
The nasal valve problem is often overlooked. Valve-related obstruction can be mistaken for swelling (rhinitis), enlarged turbinates, or a deviated septum. Multiple issues can coexist—so reducing swelling may help some, but not fully solve a structural narrowing or collapse.¹,²
A practical example: you might feel 30–50% better with allergy control but still feel “pinched” during exercise or lying down. That leftover blockage is where the valve question becomes important.
Even when scans and allergy care look “good,” a narrow or weak nasal valve can keep breathing feeling blocked.
What Is the Nasal Valve? (Simple Anatomy That Explains a Lot)
The nasal valve is the “bottleneck” of nasal airflow—already narrow, so even mild narrowing or weakness can noticeably reduce airflow.¹ Many people describe it as “the entrance caves in when I try to breathe in,” a classic clue of structural limitation.
Internal vs external nasal valve:
- Internal valve region: deeper inside, influenced by the septum and upper lateral cartilage.
- External valve region: closer to the nostril opening, influenced by the nostril rim and sidewall support.
Obstruction patterns:
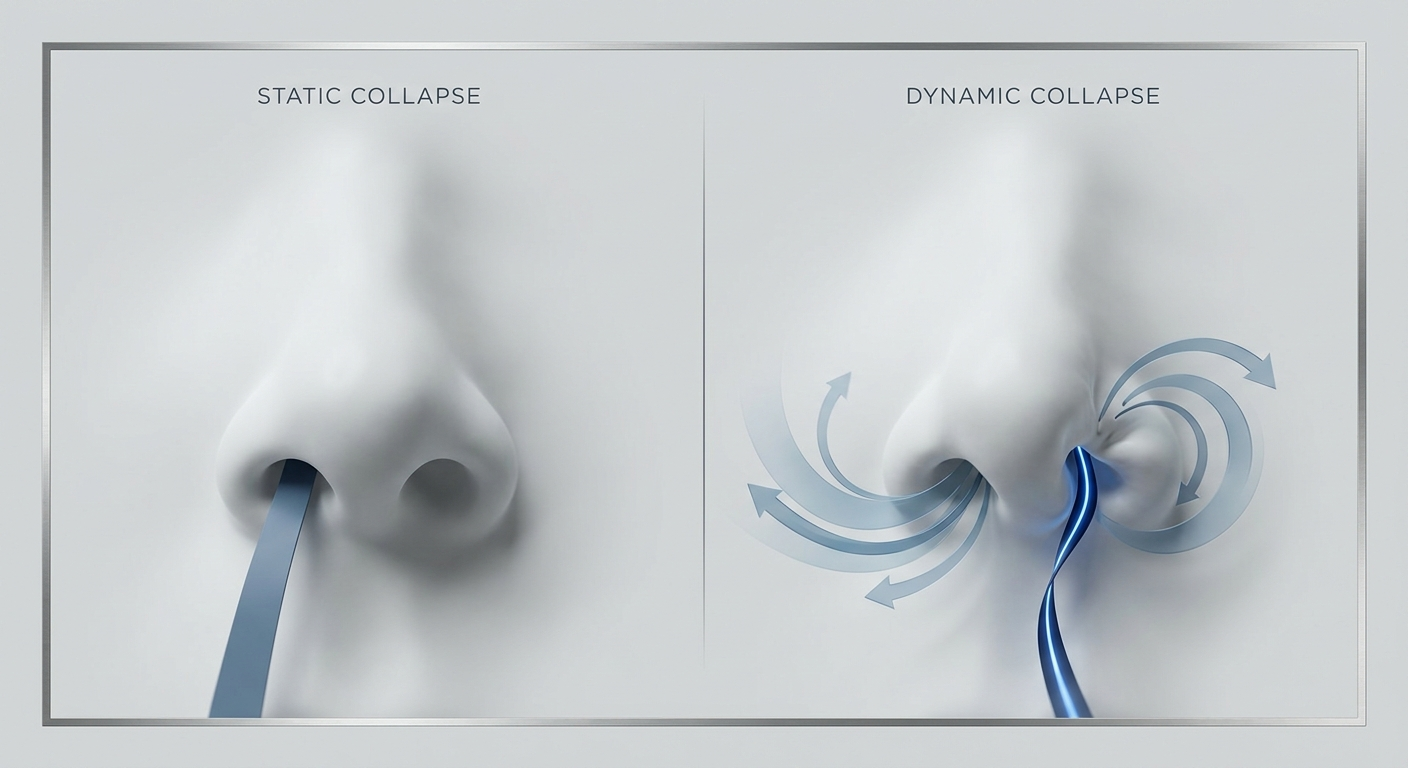
- Static: narrow all the time.
- Dynamic: collapses more during a deep breath, exercise, or sleep due to stronger negative pressure.¹
Helpful feel: static issues feel persistently tight; dynamic issues feel “okay at rest” but worse the harder you inhale.
The valve is the airway’s bottleneck—so small changes there can have big breathing effects.
Symptoms of Nasal Valve Collapse (and How It Can Affect Sleep)
Common symptoms:
- Difficulty breathing through the nose (often worse on one side).
- A feeling of “air hunger” despite little mucus.
- Blockage that worsens with deep inhaling or exertion.
- Mouth breathing and dry mouth on waking.
- Reduced exercise tolerance or feeling like you have to “pull” air in.
People often say: “I can breathe out fine, but breathing in feels blocked.” That inhale-heavy pattern points to valve function.
Visual clues:
- The nasal sidewall pulling inward during inhale.
- Narrow nostrils or asymmetry.
- Worse when lying down.
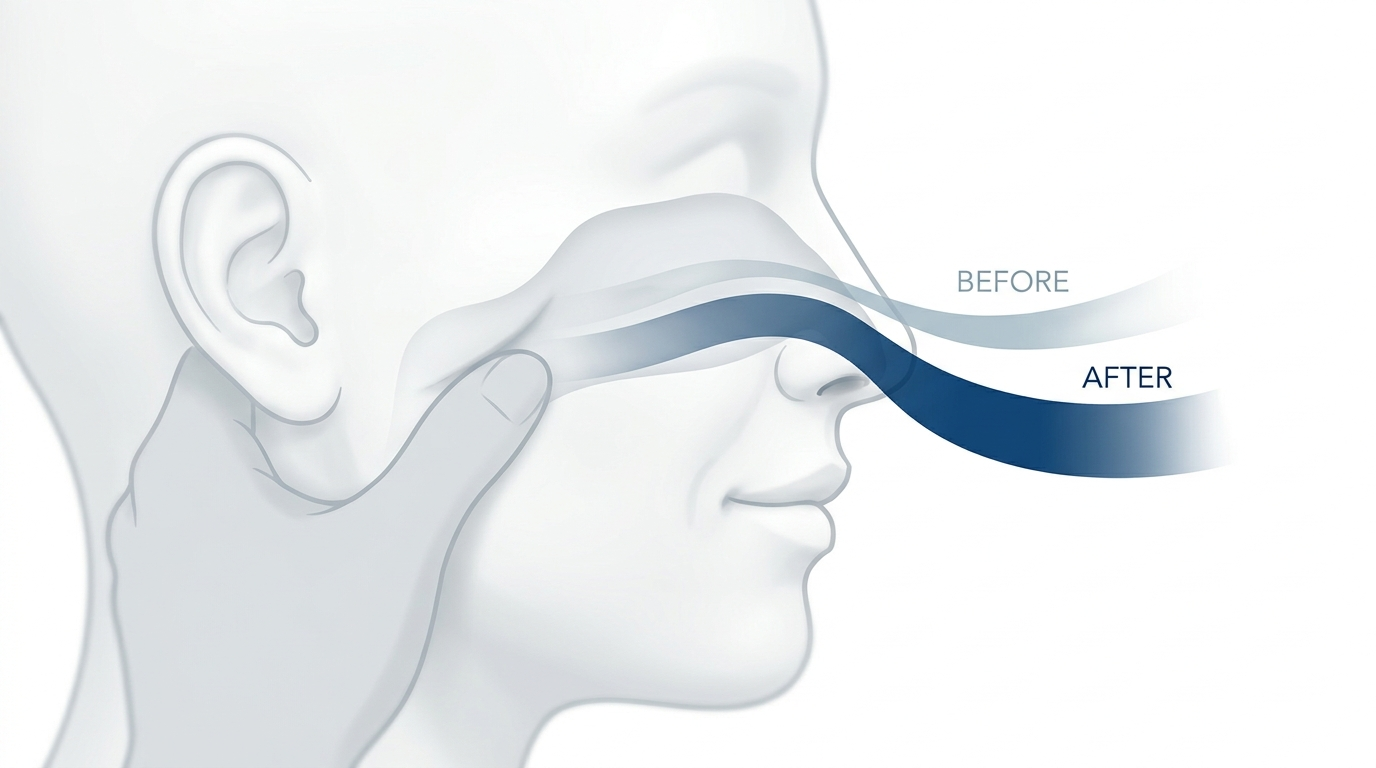
If you manually widen the nostril with a finger and breathe better, that hints at sidewall support issues.
Sleep impact: rising nasal resistance increases mouth breathing, dry throat, snoring, and fragmented sleep. It may also make CPAP harder to tolerate.³ More at: https://sleepandsinuscenters.com/blog/nasal-valve-collapse-cpap-issues-ent-solutions
If inhaling feels especially restricted—and sleep or exercise makes it worse—the valve may be involved.
Causes & Risk Factors: Why the Valve Narrows or Collapses
Structural contributors: naturally narrow anatomy and thinner sidewall support more prone to inward movement.¹ Two people can have the same mild swelling, but the one with a narrower valve feels more obstructed.
Prior injury or surgery: nasal trauma or rhinoplasty can reduce structural support, a known cause of valve collapse.¹,²
Aging: cartilage and soft-tissue support can weaken over time, increasing dynamic collapse.¹
Inflammation can “unmask” the problem: if the valve is borderline narrow, added swelling (allergy, cold) can tip airflow from “okay” to “struggling.”²
A borderline-narrow valve plus even mild swelling can tip breathing from “okay” to “struggling.”
Why It’s Misdiagnosed (and What It’s Commonly Mistaken For)
“It’s just allergies” vs mechanical narrowing: meds may reduce swelling but can’t strengthen weak sidewalls or widen a structurally narrow segment.² Partial improvement that remains worse with deep breathing suggests more than inflammation.
Deviated septum vs valve dysfunction: they can coexist. Persistent obstruction after septoplasty can be valve-related.¹ Explore more topics: https://sleepandsinuscenters.com/blog/
Turbinate swelling vs valve collapse: turbinate enlargement feels “congested” deeper inside; valve collapse feels like inhale-limited airflow, especially on deep breaths.² Many patients have a mix.
Pinpointing the true bottleneck helps target the fix.
How ENTs Diagnose Nasal Valve Dysfunction
In-office evaluation typically includes symptom pattern, external inspection while breathing, and internal exam (often with endoscopy) to assess anatomy and inflammation.
You may be asked to take stronger breaths while the clinician watches the sidewall; visible inward draw paired with your symptoms is informative.¹
Cottle maneuver: gently pulling the cheek outward to widen the sidewall area. If breathing improves, it suggests valve involvement.¹,⁴ It’s a helpful clue but not the sole planning factor.
Self-test info: https://sleepandsinuscenters.com/blog/nasal-valve-collapse-self-test-how-to-diagnose-nasal-obstruction-at-home. Self-testing can be inaccurate and should not delay professional evaluation.
Additional tools: endoscopy for inflammation/turbinates; photos/video to document dynamic movement; sometimes objective airflow tests in specialized settings.¹
Bottom line: the visit maps what limits airflow—septum, turbinates, valve (internal/external), inflammation—or a combination.
Diagnosis focuses on mapping the true airflow bottleneck so treatment matches your anatomy.
Treatments That Actually Help (From Simple to Surgical)
Treatment depends on severity, anatomy, and whether the problem is dynamic, static, or both.¹
Non-surgical options:
- External nasal dilator strips (nasal strips) for mild-to-moderate symptoms or as a “support trial.”¹,⁵
- Internal/external nasal dilators (cones) to mechanically support the nostril area.
- If inflammation contributes, address rhinitis (saline, prescribed sprays) while noting that reducing swelling doesn’t repair structural collapse.² Practical comparison: https://sleepandsinuscenters.com/blog/nasal-strips-vs-internal-dilators-which-is-best-for-better-breathing
Office-based/minimally invasive:
- Absorbable lateral wall implant (e.g., LATERA) to support the sidewall and reduce dynamic collapse in selected patients.³
Surgical options:
- Spreader graft to widen/strengthen the internal valve region, often within functional rhinoplasty.¹,²
- Other reinforcement techniques (e.g., alar batten grafts) depending on collapse location.¹
- Often combined with septoplasty and/or turbinate reduction to address multiple contributors.¹
Choosing the right option considers symptom severity, dynamic vs constant pattern, prior surgery, cosmetic considerations, and response to mechanical support. A stepwise approach is common.¹
Many people start with simple support—and pursue structural fixes if symptoms persist.
Lifestyle Tips to Breathe Easier While You’re Getting Evaluated (or While Treating)
Nighttime: short trial of a nasal strip; add humidification if dryness; some people do better on their side than their back—mention position dependence to your clinician.
Exercise/workday: a dilator during workouts may help; reduce irritant/allergen exposure to limit added swelling on top of a narrow area.²
CPAP comfort: if nasal breathing limits CPAP tolerance, consider early valve evaluation—sometimes the nasal “front end” is the limiting factor.³
Small day-to-day adjustments can reduce “added resistance” while you pursue a definitive fix.
When to See an ENT (Red Flags & Timing)
Make an appointment if you have: nasal obstruction lasting several weeks despite treatment; persistent one-sided obstruction; snoring, mouth breathing, or sleep disruption linked to nasal blockage; prior nasal trauma or rhinoplasty followed by new breathing difficulty.¹,²
Sleep and Sinus Centers of Georgia can help evaluate whether valve dysfunction is part of the picture: https://www.sleepandsinuscenters.com/
Seek urgent care for severe bleeding, facial swelling with fever, vision changes, or sudden severe worsening symptoms.
If stubborn blockage is affecting daily life or sleep, it’s reasonable to get a focused nasal breathing evaluation.
FAQs About Nasal Valve Collapse
What does it feel like? Often like you can’t get enough air in through the nose—especially during a deep breath—without much mucus.
Can it cause snoring or poor sleep? It can contribute by increasing mouth breathing and nasal resistance.³
How do I test it at home (is the Cottle safe)?¹,⁴ A gentle cheek pull can hint at improvement, but it’s only a clue. Don’t delay professional care.
Do nasal strips work?¹,⁵ They can help in mild-to-moderate cases or at night and serve as a quick support trial.
Is it the same as a deviated septum?¹ No—different problems that can coexist.
Will steroid sprays fix it?² They reduce swelling but don’t strengthen cartilage or sidewall support.
What is a spreader graft?¹,² Cartilage used to widen/strengthen the internal valve region.
What is a LATERA implant?³ An absorbable implant designed to support the lateral wall and reduce dynamic collapse in selected patients.
Can it come back after treatment?¹ Outcomes depend on anatomy, tissue strength, healing, and whether all obstruction sites were addressed.
Conclusion: Restoring Valve Function Can Be the Missing Piece
Because the nasal valve is the main airflow bottleneck, dysfunction there is a common reason people feel persistently blocked—even when other treatments don’t fully work.¹ Options range from nasal strips and minimally invasive support to reconstructive approaches like spreader grafts or absorbable implants.¹,³ If ongoing nasal obstruction affects your sleep, workouts, or CPAP comfort, consider a nasal breathing evaluation with Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Sources
1. https://pmc.ncbi.nlm.nih.gov/articles/PMC9450767/
2. https://pmc.ncbi.nlm.nih.gov/articles/PMC4158473/
3. https://pmc.ncbi.nlm.nih.gov/articles/PMC11375169/
4. https://pmc.ncbi.nlm.nih.gov/articles/PMC12761343/
5. General patient education summaries referenced in the outline
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.






