
Jaw Surgery for Sleep Apnea (MMA): Benefits, Risks & Recovery Timeline
Medical disclaimer: This article is for general education only and isn’t a substitute for medical advice, diagnosis, or treatment. Your situation may be different—use this as a starting point for a discussion with your sleep and surgical team.
Introduction — When Sleep Apnea Treatment Needs More Than CPAP
Obstructive sleep apnea (OSA) is more than snoring. It can fragment your sleep, lower oxygen levels overnight, and contribute to daytime fatigue, headaches, and reduced concentration. Over time, untreated OSA is associated with increased health and safety risks—especially when sleepiness affects driving or work.
For many people, CPAP is highly effective. But it’s not always tolerated, and some patients continue to have symptoms despite consistent use. In those cases, jaw surgery for sleep apnea—most commonly maxillomandibular advancement (MMA)—may be part of the discussion. MMA is widely regarded in the literature as one of the most effective surgical treatments for appropriately selected patients with moderate-to-severe OSA, with strong, consistent reductions in apnea severity across studies [1,3].
Clinicians often frame the decision this way: CPAP “splints” the airway open with air pressure, while MMA changes the underlying anatomy to create more room for airflow. Surgery isn’t the right next step for everyone, and a thorough evaluation matters.
Conclusion: MMA may be a powerful option when anatomy and severity align, but it should be considered within a comprehensive, personalized plan.

Sleep Apnea Basics (Patient-Friendly)
Common symptoms of obstructive sleep apnea
- Loud, frequent snoring
- Choking/gasping during sleep or witnessed pauses in breathing
- Excessive daytime sleepiness, fatigue, or “brain fog”
- Morning headaches, dry mouth, or sore throat
- Mood changes (irritability, low motivation)
- Trouble concentrating or memory issues
A practical example: someone might “sleep” 8 hours but still feel drained because the brain keeps partially waking up to reopen the airway. A bed partner may notice the breathing pauses long before the patient feels concerned.
What causes the airway to collapse during sleep?
OSA happens when airflow is repeatedly blocked during sleep—often because the space behind the tongue and soft palate is too narrow or becomes “floppy” when muscles relax at night.
Contributors can include:
- Soft tissue crowding behind the tongue/soft palate
- Jaw position and airway anatomy (skeletal structure can influence airway size)
- Weight changes, alcohol/sedatives, and nasal obstruction (which may worsen airflow or sleep quality)
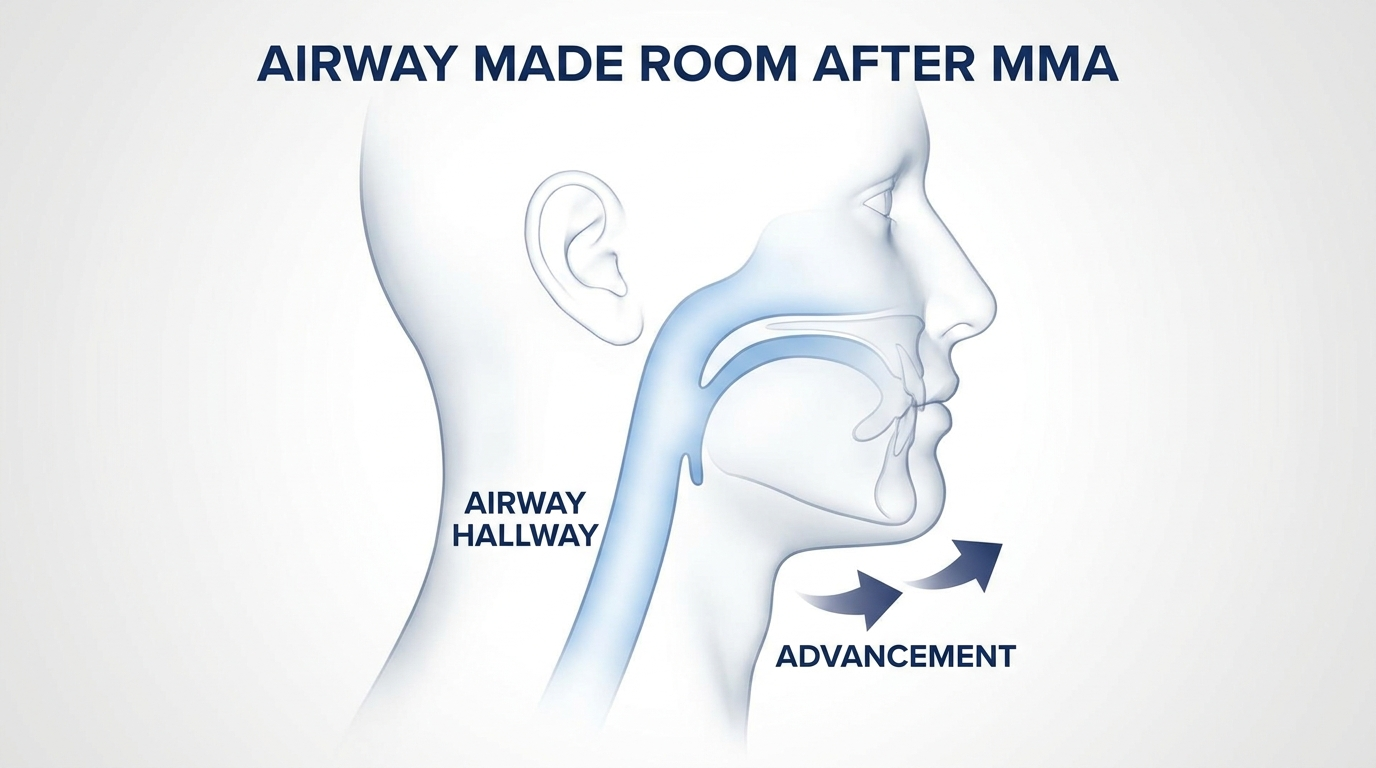
A helpful analogy: if your airway is like a hallway, soft tissues are the “furniture,” and the jaws are part of the “walls and frame.” CPAP pushes air through the hallway; MMA can widen the frame itself so airflow has more space.
If you’d like a quick primer on how severity is measured, see our guide: AHI score explained: understanding your sleep apnea severity — https://sleepandsinuscenters.com/blog/ahi-score-explained-understanding-your-sleep-apnea-severity
Conclusion: Understanding your symptoms and AHI basics can make consultations more productive.
What Is “Jaw Surgery for Sleep Apnea”?
MMA explained in plain language
When people refer to jaw surgery for sleep apnea, they’re often talking about maxillomandibular advancement (MMA). MMA surgically moves the upper jaw (maxilla) and lower jaw (mandible) forward. That forward shift helps enlarge the airway—especially the space behind the tongue and soft palate, where collapse commonly occurs [1,3]. Because the tongue attaches to the lower jaw, advancing the jaws tends to bring key soft tissues forward as well—often helping reduce collapsibility in the areas most commonly involved in OSA.
How MMA differs from other sleep apnea surgeries
Many OSA procedures target soft tissues (like the palate). MMA is different because it targets the skeletal structure, which can have a larger, more predictable effect on airway size and shape.
It’s often considered when:
- CPAP isn’t tolerated or isn’t helping enough, or
- A person’s anatomy suggests skeletal advancement could meaningfully improve airflow
In real life, the “why MMA?” conversation often comes up when a patient says something like: “I know CPAP works, but I can’t sleep with it,” or “I’m using it and still feel exhausted.” MMA is one of the most evidence-supported surgical options when anatomy and severity line up.
Conclusion: MMA alters airway structure rather than soft tissue alone, which can translate to larger, more durable airflow gains for the right patient.

How Effective Is MMA for Obstructive Sleep Apnea?
Success rates and AHI improvement (what the numbers mean)
The AHI (Apnea-Hypopnea Index) is the number of breathing disruptions per hour of sleep. In general, lower AHI means fewer events and typically better oxygen stability and sleep quality.
Reported outcomes after MMA include:
- Up to 83.4% of patients achieving AHI ≤ 15 events/hour in some cohorts [1]
- About 46.7% reaching an AHI < 5, often considered within the normal range [1]
- Overall “surgical success” across studies commonly ranging ~57%–86%, depending on how success is defined and which patients are included [2]
A key nuance: “success” is not always defined the same way from study to study. Some definitions focus on reaching a specific AHI threshold, while others require a certain percentage reduction from baseline. Your surgeon can explain which benchmark best matches your goals and starting severity.
Why MMA is often considered among the most effective surgical options for moderate-to-severe OSA
Across multiple studies and reviews, MMA tends to produce large, durable reductions in AHI—especially compared with many soft-tissue-focused surgeries [1-3]. For patients exploring CPAP alternatives, this consistency is part of why MMA is frequently described as one of the most effective surgical approaches for appropriately selected patients with moderate-to-severe disease.
Conclusion: Outcomes vary, but MMA consistently shows substantial AHI reductions across diverse patient groups.

Who Is a Good Candidate for MMA?
Situations where MMA may be recommended
MMA may be considered for people with:
- Moderate-to-severe OSA, persistent symptoms, or significant oxygen drops
- CPAP intolerance or inadequate benefit despite good effort
- Airway crowding that appears related to jaw position/anatomy on exam and imaging
A concrete example: a patient with moderate-to-severe OSA who repeatedly removes CPAP during sleep or can’t tolerate pressures may ask about long-term options. If the airway exam and imaging suggest skeletal restriction, MMA may rise on the list of interventions to discuss.
If you’re earlier in the process, it may help to review OSA testing options: home sleep test vs. lab study — https://sleepandsinuscenters.com/blog/home-sleep-test-vs-lab-study-which-sleep-test-is-best-for-you
Pre-surgery evaluation checklist
- Review of a recent sleep study (AHI, oxygen levels, symptoms)
- Airway evaluation and imaging (often CT/CBCT or cephalometric planning)
- Dental/orthodontic assessment to plan how the bite will fit after advancement
- Discussion of alternatives, likely outcomes, and what “success” means (numbers, symptoms, or both)
This is where planning gets personalized. Some people need coordinated orthodontic planning to ensure the bite functions well after the jaws are advanced. Others may already have an alignment that can be managed with less orthodontic involvement.
Who may need extra caution (not always a “no,” but needs discussion)
- Uncontrolled medical conditions (for example, poorly controlled diabetes)
- Smoking/vaping
- Significant cardiac or pulmonary risk factors that require careful anesthesia planning
Conclusion: A thorough, team-based evaluation helps match the right patients to the right procedure at the right time.
Benefits of Jaw Surgery for Sleep Apnea (Beyond Snoring)
Breathing and sleep improvements
Potential benefits reported after MMA include:
- Fewer apneas/hypopneas and improved oxygen levels
- Less sleep fragmentation and better daytime alertness
Because MMA aims to enlarge the airway in a mechanically meaningful way, improvements often show up both in sleep study results and in day-to-day functioning—though the degree of improvement varies person to person.
Quality-of-life benefits many patients report
When OSA improves, people often notice:
- Less fatigue and better mental clarity
- Reduced snoring (often significant)
- Improved sleep-related quality of life, which may support long-term wellness
A patient-style comment you might hear is: “I didn’t realize how foggy I felt until I started waking up clearer.” It can be subtle at first, then more obvious as recovery progresses and sleep stabilizes.
When MMA may reduce the need for CPAP
Some patients may no longer need CPAP after MMA, while others may still need it or use lower pressures [3]. Individual results vary, and follow-up testing is often used to confirm the outcome.
For additional context on non-CPAP paths, see: Is your CPAP machine getting in the way? — https://sleepandsinuscenters.com/is-your-cpap-machine-getting-in-the-way
Conclusion: Many patients experience meaningful symptom relief after MMA, with CPAP needs varying based on final AHI and symptoms.
Risks and Potential Complications of MMA (Clear, Non-Alarming)
Common/expected short-term effects
Many people experience:
- Swelling, bruising, and soreness
- Temporary difficulty chewing (diet changes are expected)
- Nasal congestion and disrupted sleep early on
It can help to anticipate that the first couple of weeks are often the most inconvenient, even when pain is well controlled—mostly because swelling, congestion, and diet limitations can affect sleep and energy.
Medical and surgical risks to review with your surgeon
As with other major surgeries, topics to discuss include:
- Bleeding or infection
- Jaw healing issues (delayed union/nonunion—uncommon but important)
- Bite changes that may require orthodontic adjustments
- Temporomandibular joint (TMJ) discomfort or muscle tightness during recovery
Your team may also talk through how these risks are monitored—follow-up visits, imaging when needed, and specific instructions that protect healing in the early phase.
Nerve-related risks (important patient question)
Altered sensation or numbness—often in the lower lip or chin—can occur. It frequently improves over time, but some degree of change may persist in a subset of patients.
Aesthetic changes (often part of the decision)
Because MMA moves the jaws forward, it can change facial appearance (often most noticeable in the profile). This is neither “good” nor “bad” universally—it’s simply important to plan for and discuss in advance.
Conclusion: Knowing the likely benefits and risks up front supports realistic expectations and safer recovery.

What Recovery From MMA Looks Like (Timeline Guide)
Recovery varies based on the surgical plan, individual healing, and whether orthodontics is involved, but a general timeline looks like this:
Immediately after surgery (first 24–72 hours)
- Close monitoring, swelling management, and a pain-control plan
- Fatigue is common
- Comfort strategies often include head elevation and hydration (as directed by your surgical team)
Many patients describe this stage as “sleepy and swollen.” Your job is mostly rest, hydration, and following the medication and oral-care plan as directed by your surgical team.
Week 1–2: the “swelling and routine” phase
- Liquid or very soft diet is typical
- Oral hygiene instructions are important (your team will outline what’s safe)
- Many people plan time off work/school due to swelling and low energy
If you’re planning ahead, this is usually the period when meal prep matters most—many patients find that protein-forward liquids and soft foods make a noticeable difference in how steady their energy feels.
Weeks 3–6: gradual return to normal activities
- Soft foods are usually advanced slowly
- Light activity typically increases as tolerated
- Follow-up visits focus on bite alignment and healing progress
This is often when people start saying, “I feel more like myself,” even though full healing is still in progress.
2–3 months and beyond: longer-term healing
- Bone healing and bite stabilization continue
- A follow-up sleep test may be discussed to document AHI reduction and guide any remaining therapy
If you’re wondering about timing for post-treatment testing, this article may help: when to repeat a sleep study: key signs and timing explained — https://sleepandsinuscenters.com/blog/when-to-repeat-a-sleep-study-key-signs-and-timing-explained
Conclusion: Expect the biggest day-to-day improvements after the early swelling phase, with formal outcome checks once healing stabilizes.
Preparing for Jaw Surgery (Practical Pre-Op Tips)
Questions to ask at your consult
- How much advancement is planned—and why?
- What’s the goal: symptom relief, a specific AHI target, or both?
- What is the plan if residual OSA remains?
- What does your typical recovery timeline look like?
You can also ask who will be involved in planning (sleep medicine, orthodontics, oral-maxillofacial surgery) and how follow-up testing is handled after you’ve healed.
Home and work planning
- Arrange help for the first few days
- Stock high-protein liquids and soft foods ahead of time
- Set up a comfortable sleep space (often with head elevation)
A small but practical tip: plan for more time than you hope you’ll need. If you feel great sooner, that’s a bonus.
Nutrition and habits that support healing
- Prioritizing protein and hydration
- Avoiding smoking/vaping
- Reviewing medications/supplements with your surgical team (especially anything that affects bleeding)
Conclusion: A little planning up front can make early recovery smoother and safer.

Alternatives to MMA (So Patients Understand the Full Menu)
CPAP/APAP (first-line for many patients)
CPAP remains the standard first-line treatment for many people because it can work extremely well. Challenges can include mask discomfort, dryness, and adherence.
Oral appliance therapy (mandibular advancement device)
Oral appliances can be effective in selected patients, often those with mild-to-moderate OSA. Learn more: oral appliance vs CPAP: which is right for you — https://sleepandsinuscenters.com/blog/oral-appliance-vs-cpap-which-is-right-for-you
Inspire / hypoglossal nerve stimulation (for qualifying patients)
This option may be considered for people who meet specific criteria related to OSA severity and airway anatomy. Overview: Inspire hypoglossal nerve stimulation: a 101 guide to sleep apnea treatment — https://sleepandsinuscenters.com/blog/inspire-hypoglossal-nerve-stimulation-a-101-guide-to-sleep-apnea-treatment
Other surgeries and procedures
Depending on anatomy, other procedures may be discussed, such as palate-focused surgery or nasal surgery to improve airflow (often to support breathing comfort or CPAP tolerance rather than “cure” OSA).
For an overview of evaluation and treatment pathways, visit: Snoring & sleep apnea treatment — https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
Conclusion: Reviewing all options helps you balance effectiveness, recovery, and long-term fit for your lifestyle.
Lifestyle Tips That Can Improve Outcomes (With or Without Surgery)
Even when surgery is part of the plan, lifestyle factors can still matter:
- Sleep position: Side sleeping helps some people; elevation may help when reflux or congestion contributes.
- Alcohol/sedatives: These can worsen airway collapse in some individuals.
- Nasal breathing support: Treating allergies and nasal obstruction may improve sleep quality and comfort.
Conclusion: Small habit changes can complement any primary OSA therapy and may improve day-to-day sleep quality.
FAQs About Jaw Surgery for Sleep Apnea (MMA)
Is MMA really among the most effective surgeries for sleep apnea?
For moderate-to-severe OSA, MMA is often described in the medical literature as one of the most effective surgical approaches because it consistently produces substantial AHI reductions across studies [1-3].
Will MMA cure my sleep apnea?
Many people improve dramatically, and some reach AHI levels often considered within the normal range, but others have residual OSA and may still need therapy [1,2]. A follow-up sleep study helps clarify the outcome.
How long will I be on a liquid/soft diet?
Many patients spend at least 1–2 weeks on liquids/very soft foods, then gradually advance over several weeks. Exact timing varies by surgeon and healing progress.
Is the recovery painful?
Discomfort is expected, but many people report swelling and congestion are bigger issues than pain after the first few days. Your surgical team typically provides a detailed plan.
Will my face look different?
Usually, yes—because the jaws move forward. This should be discussed in planning so expectations match likely results.
When can I return to work/exercise?
Return-to-activity timing varies. Some people return to desk work in a few weeks; heavier physical activity typically takes longer and depends on clearance from the surgical team.
Do I need a follow-up sleep study after MMA?
Often, yes—especially to document AHI reduction and decide whether any additional therapy is needed.
When to Seek Medical Help After Surgery (Safety Box)
Contact your surgical team urgently if you experience:
- Fever, worsening redness, or drainage
- Uncontrolled bleeding
- Breathing difficulty beyond expected swelling
- Severe or worsening pain not controlled by prescribed medication
- Signs of dehydration or inability to keep nutrition down
Conclusion — Next Steps If You’re Considering MMA for Sleep Apnea
If CPAP hasn’t been workable and you’re exploring jaw surgery for sleep apnea, MMA may offer an anatomy-based way to widen the airway and reduce apnea severity. It’s also a major procedure with real recovery demands—so it’s worth taking time to understand the full picture, including alternatives and realistic goals (symptoms and AHI reduction).
A comprehensive evaluation is the best way to learn whether maxillomandibular advancement (MMA) fits your airway anatomy, sleep study findings, and preferences. This type of surgery is typically performed by specialized oral-maxillofacial surgeons, working in coordination with sleep and dental teams when needed.
To explore options and book an appointment, visit https://www.sleepandsinuscenters.com/ and start with Snoring & sleep apnea treatment — https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
Conclusion: The right next step is a thorough consult that aligns treatment with your goals, anatomy, and lifestyle.
References
1. Maxillomandibular advancement outcomes (AHI response rates). https://pmc.ncbi.nlm.nih.gov/articles/PMC4481052/
2. MMA success rate ranges across cohorts (2024). https://www.sciencedirect.com/science/article/abs/pii/S0266435624005199
3. Patient-facing overview of MMA for OSA. https://www.rush.edu/maxillomandibular-advancement-surgery-treatment-obstructive-sleep-apnea
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.





