Trouble Breathing Through Nose: Causes, Symptoms, and Treatments
Introduction — When a “stuffy nose” is more than an annoyance
A nose that won’t clear can affect more than comfort. Many people notice sleep disruption, reduced exercise tolerance, frequent mouth breathing, headaches, or feeling “foggy” during the day. Trouble breathing through the nose is often a sign of nasal obstruction—reduced airflow through one or both nostrils—and it’s a common reason people seek care.
The encouraging news: many cases of nasal obstruction are caused by reversible inflammation (like allergies or chronic rhinitis). Other cases are structural, such as a deviated septum, turbinate hypertrophy, or nasal polyps, which may require an ENT evaluation to fully diagnose and treat. Sources like EPOS 2020 and Cleveland Clinic emphasize this “inflammation vs. structure” framework because it helps guide what treatments are most likely to help. [1][3]
A helpful way to picture it: inflammation is like the “lining” of the nose swelling (puffy tissue narrowing the airway), while structural problems are more like the “frame” being narrow or crooked. Many people have a mix of both, so treatment plans often target inflammation and anatomy together.
Bottom line: understanding whether your blockage is driven by inflammation, structure, or both is the key to an effective plan.

What does “trouble breathing through your nose” feel like?
Common ways patients describe it
- “One side is always blocked.”
- “I have nasal congestion that never fully clears.”
- “I can’t breathe through my nose at night.”
- A sense of pressure/fullness, reduced smell, snoring, or chronic mouth breathing
Some people describe it as “breathing through a straw,” especially when exercising or lying down. Others say they can breathe “fine” during the day but feel blocked the moment their head hits the pillow. If you’ve had trouble breathing through the nose for a while, these details (especially one-sided vs. both sides) can be important for narrowing down likely causes.
Acute vs. chronic nasal obstruction (why the timeline matters)
- Acute (days to <4 weeks): often a viral cold, an irritant exposure, or an allergy flare. [3]
- Chronic (≥12 weeks): more suggestive of chronic rhinitis, chronic rhinosinusitis (CRS), nasal polyps, turbinate hypertrophy, deviated septum, or nasal valve problems. [1][3]
If your symptoms come in waves (better some days, worse others), that can still be “chronic”—especially if the overall pattern persists for months.
In short, note which side feels blocked and how long it’s been happening—those two clues go a long way.
Symptoms to watch for (and what they may suggest)
Typical symptoms
- Blocked airflow or persistent nasal congestion
- Runny nose (clear vs. thick) and post-nasal drip
- Sneezing/itching (often points toward allergic rhinitis)
- Facial pressure, reduced smell/taste
- Mouth breathing, dry mouth, snoring, and poor sleep quality [3]
A simple self-check many clinicians use: if congestion comes with itching/sneezing and clear drainage, allergies move up the list. If it comes with reduced smell and long-lasting blockage, CRS or polyps become more likely. These aren’t diagnoses by themselves—but they’re useful clues.
Red flags — seek urgent care or prompt ENT evaluation
- Sudden severe blockage after an injury
- Unilateral (one-sided) blockage with recurrent nosebleeds, foul odor, or a visible mass
- Fever with worsening facial swelling or severe headache
- Eye swelling, vision changes, stiff neck, or confusion (rare but urgent complications related to sinus disease) [1][3]
One ENT-style rule of thumb: when symptoms are one-sided, new, and persistent—don’t just “wait it out.” It’s usually benign, but it’s worth checking.
Use symptom clusters (e.g., itch/sneeze vs. smell loss) to guide likely causes—and act quickly on red flags.

Causes of nasal obstruction (most common reasons)
A helpful way to think about trouble breathing through the nose is to separate causes into inflammation (often reversible) and structural/mechanical blockage. [3] Many people have both—say, a mild septal deviation plus seasonal allergies—so a plan often needs to address inflammation and anatomy.
Inflammatory causes (most common)
Allergic rhinitis (seasonal or year-round)
Allergic rhinitis is triggered by pollen, dust mites, pets, or mold. Classic clues include sneezing, itching (nose/eyes), and clear drainage—often alongside nasal congestion. [3]
A concrete example: you may feel fine at work, but get congested at home (pet dander), or feel reliably worse during spring or fall (pollen). When symptoms track exposures like that, allergy-focused treatment is more likely to pay off.
Nonallergic (vasomotor) rhinitis
Nonallergic rhinitis can be triggered by weather changes, strong smells/fragrances, smoke, spicy foods, or certain medications. It tends to cause more congestion and drip, and less itching/sneezing than allergies. [3]
For a deeper dive into chronic rhinitis treatment options, you can read: https://sleepandsinuscenters.com/treating-chronic-rhinitis
Patients often describe this as “my nose has a mind of its own”—fine one moment, streaming or congested the next—without an obvious allergy pattern.
Viral upper respiratory infection (“common cold”)
Colds can cause significant congestion that often peaks early and improves within about 7–10 days. A key point: antibiotics do not treat viral colds. [3]
It’s also common for nasal stuffiness to linger after the worst of the cold is over. That doesn’t automatically mean bacterial infection—it can reflect inflammation that simply takes longer to settle.
Acute rhinosinusitis vs. chronic rhinosinusitis (CRS)
- CRS is typically defined by symptoms lasting ≥12 weeks, along with objective evidence of inflammation on exam, endoscopy, or CT. [1]
- CRS with nasal polyps (CRSwNP) often causes more significant obstruction and reduced smell. [1][2]
If you find yourself saying, “I can’t remember the last time my nose felt clear,” that’s a classic CRS-style timeline worth discussing with a clinician.

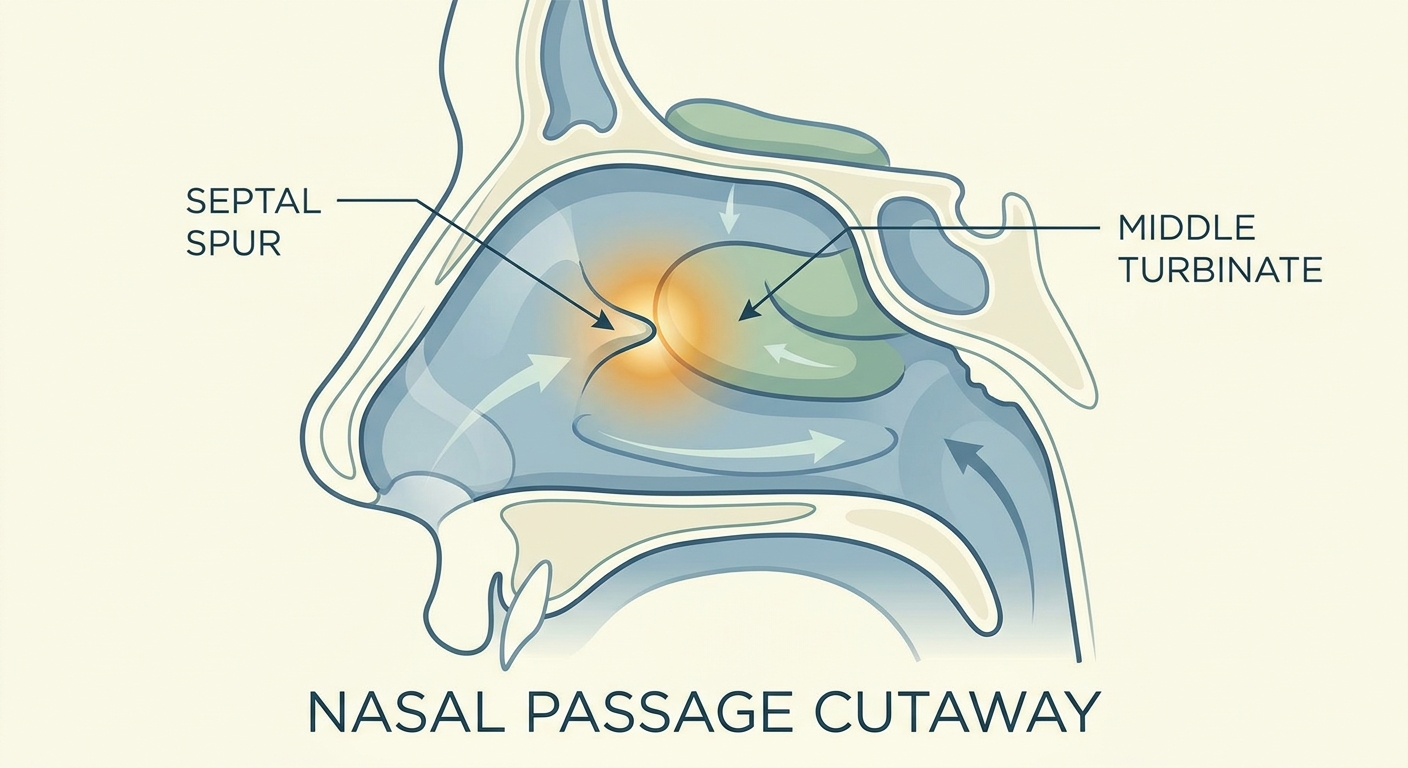
Structural (mechanical) causes
Deviated septum
A deviated septum can narrow one side of the nose and commonly causes one-sided obstruction that worsens during colds or allergy seasons. It’s also a frequent reason symptoms persist even when someone uses sprays correctly. [3]
Learn more about deviated septum symptoms and treatment: https://sleepandsinuscenters.com/deviated-septum-relief
Some patients notice they can “always” breathe better through one nostril than the other. That pattern is often structural, even if inflammation is also present.
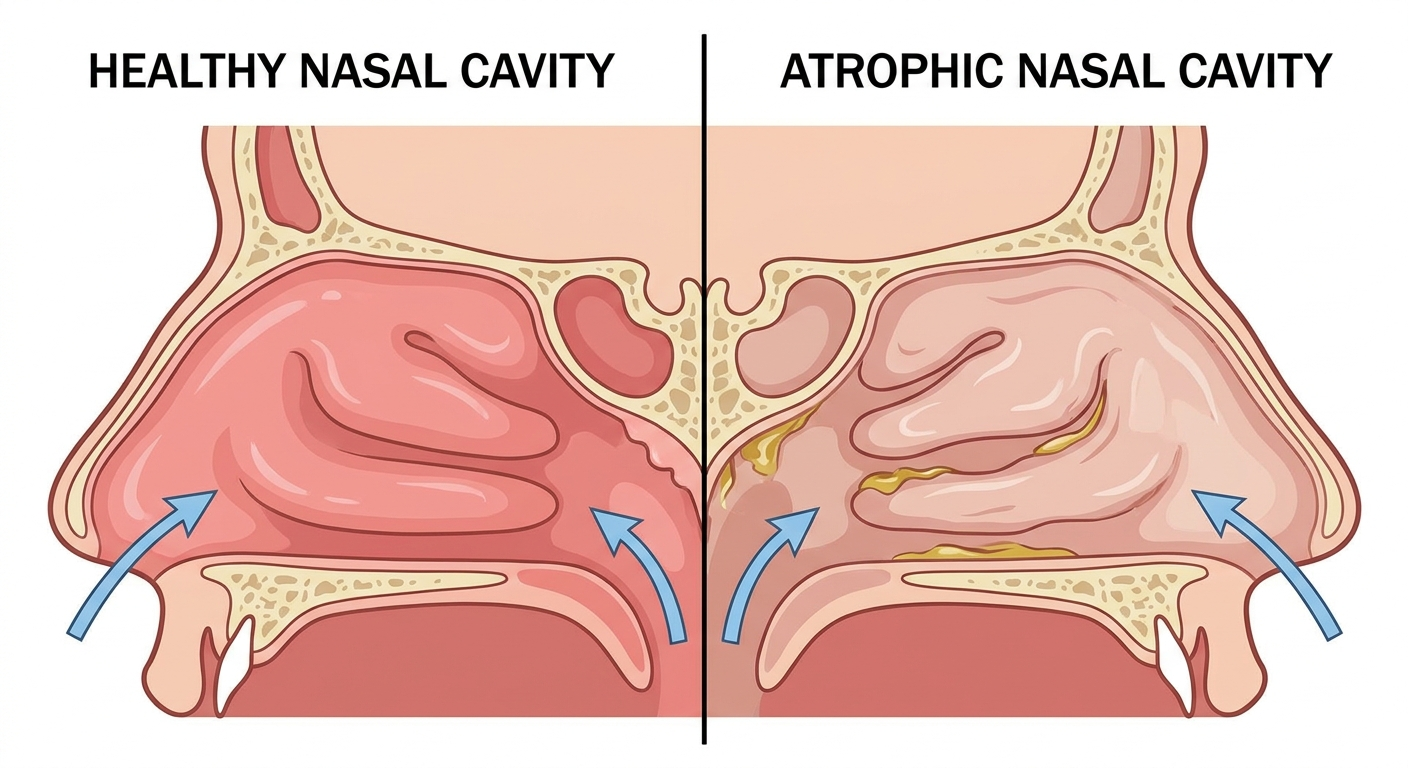
Turbinate hypertrophy
The turbinates are structures inside the nose that help humidify and filter air. When they enlarge—often due to chronic inflammation—they can significantly reduce airflow (turbinate hypertrophy). [3]
Think of turbinates like the nose’s built-in air filters. When they swell, the “filter housing” takes up more space, leaving less room for airflow.
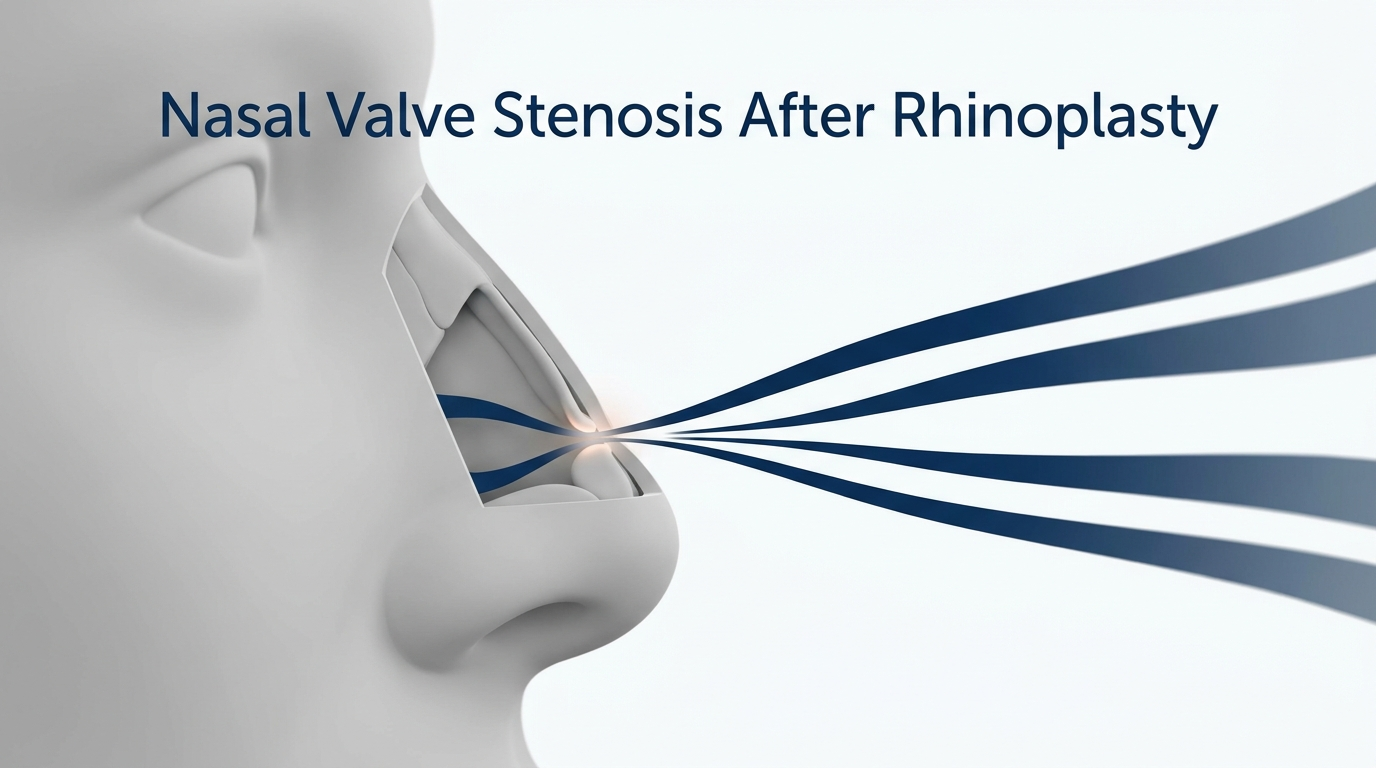
Nasal valve collapse
Some people notice the nostrils “pull inward” during inhalation, particularly with exercise or sleep. That can indicate nasal valve issues. [3]
A common clue is that lifting the cheek skin slightly to the side (or using a nasal dilator strip) temporarily improves breathing—suggesting the “doorway” of the nose is narrowing with each breath.
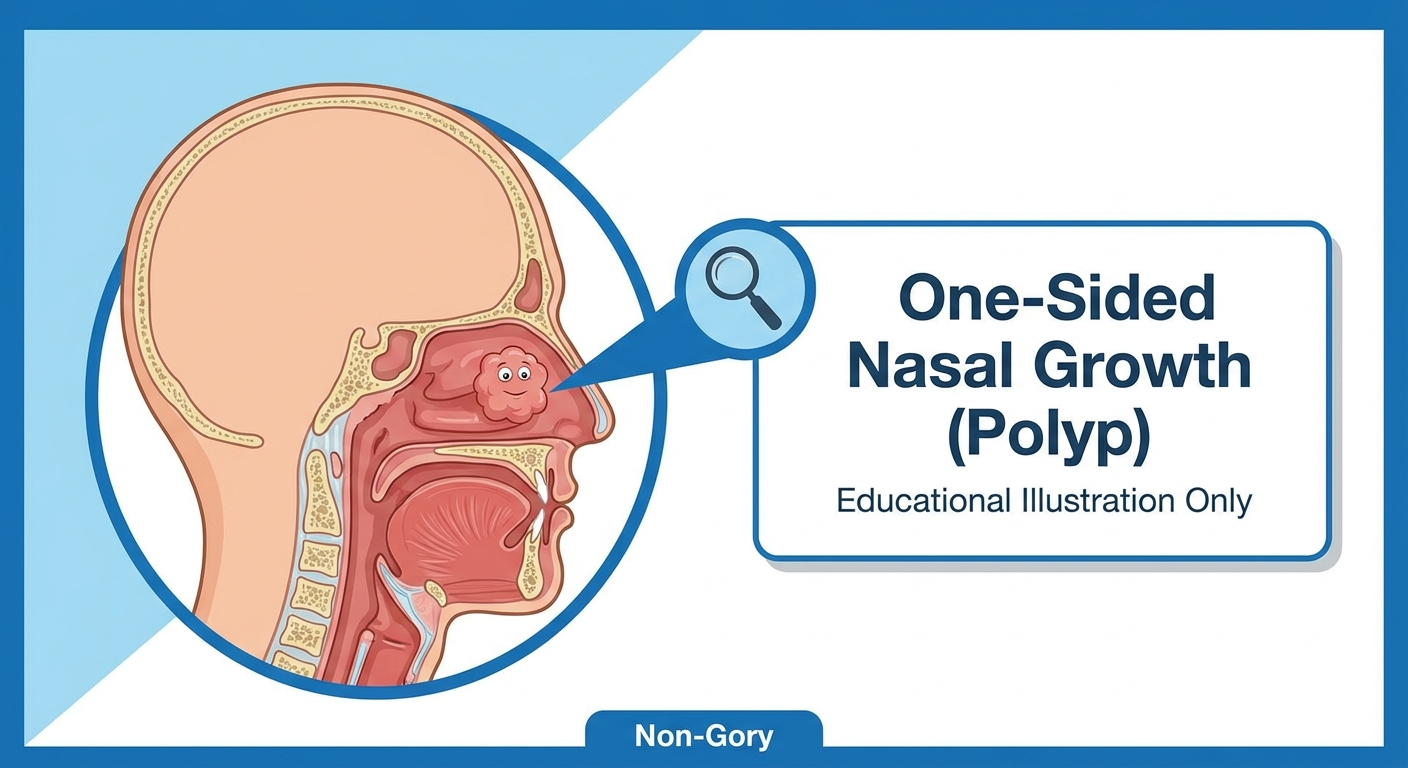
Nasal polyps
Nasal polyps are soft inflammatory growths commonly associated with CRS and type 2 inflammation. They can cause major blockage and reduced smell. [1][2]
People with polyps often report that smell fades gradually rather than suddenly, and that congestion feels “deep” or persistent despite typical OTC remedies.
Enlarged adenoids (children)
In children, enlarged adenoids can contribute to mouth breathing, snoring, nasal speech, and recurrent infections. [3]
Less common but important
- Foreign body (especially in children; one-sided foul drainage)
- Tumors (rare; persistent unilateral symptoms, especially with bleeding) [3]
Most patients have a mix of inflammatory and structural factors—successful care often addresses both.

Why it happens at night (and why you wake up mouth-breathing)
Normal nasal cycle + sleep position
The nasal cycle naturally alternates congestion from side to side. For many people it’s barely noticeable—but if baseline airflow is already narrowed (from inflammation or structure), nighttime awareness can be much stronger.
If you sleep on your right side and the right nasal passage is the “down” side, you may notice that side feels more blocked—for some people this effect is more noticeable.
Bedroom triggers
Common nighttime triggers include dust mites, pet dander, dry air, mold exposure, and fragrance/irritants. [3]
A practical example: symptoms that reliably worsen in the bedroom (but improve when traveling) can point toward an indoor trigger rather than an infection.
Reflux and sleep-disordered breathing overlap (brief mention)
Nasal obstruction can overlap with snoring and can make some sleep-disordered breathing treatments harder to tolerate. This is one reason persistent trouble breathing through the nose may be worth evaluating rather than simply “pushing through.”
Nighttime stuffiness often reflects normal physiology amplified by triggers—reducing triggers and improving baseline airflow can help.
How clinicians diagnose the cause (what to expect at an ENT visit)
History questions that narrow the diagnosis
- Is it seasonal, triggered, or constant?
- One side or both?
- Any smell changes?
- Response to medications—and whether topical decongestant sprays have been used frequently (more than 3 consecutive days can lead to rebound congestion) [3]
It can help to bring specifics: which sprays/pills you tried, how long you used them, and whether you used them daily or only during flares.
Physical exam and nasal endoscopy
- Septal deviation
- Turbinate swelling
- Polyps
- Drainage patterns suggesting sinus involvement [3]
Many patients are relieved by how much clarity a direct look provides—turning a vague “stuffy all the time” into a concrete plan.
When imaging (CT) is helpful—and when it isn’t
A CT scan is most helpful when CRS or structural disease is suspected, or when planning procedures. CRS diagnosis usually also requires objective evidence on exam, endoscopy, or CT—not symptoms alone. Routine, short-lived congestion typically does not require imaging. [1]
Allergy testing (when it changes treatment)
When symptoms are persistent or clearly triggered (seasonal or environmental), allergy testing may help guide avoidance strategies and longer-term plans. [3]
A focused history, exam/endoscopy, and selective imaging or testing usually reveal the “why” behind nasal blockage.

Treatments that actually help (step-by-step approach)
Treatment works best when it matches the cause—especially the difference between inflammation and structure.
At-home care (safe first steps)
- Saline rinse (irrigation or spray) to clear mucus and reduce irritant/allergen load [1][3]
- Humidification if dryness is a trigger
- Warm showers/steam for symptom comfort
- Trigger control (avoid smoke and strong fragrances)
A helpful way to think about saline irrigation: it doesn’t “cure” the cause, but it can lower the day-to-day burden (mucus, crusting, allergens) so other treatments work better.
Over-the-counter (OTC) options—what to use and what to avoid
Antihistamines (for allergies)
When sneezing, itching, and watery drainage are prominent, antihistamines may help (especially for allergic rhinitis). [3]
If congestion is the main symptom and itching/sneezing are minimal, antihistamines may be less noticeable—another clue you may be dealing with nonallergic rhinitis or structural narrowing.
Decongestants (short-term only)
Decongestants can offer temporary relief, but topical decongestant sprays used too long can lead to rebound congestion—often after more than 3 consecutive days. [3]
If you feel like you “can’t breathe without the spray,” that’s a sign to speak with a clinician about safer long-term options.
Proper nasal spray technique (quick how-to)
- Aim the spray slightly outward (toward the ear), not straight up the middle (septum)
- Use it consistently—many therapies help most when used regularly, not “only when miserable”
A quick clinician-style tip: spray, then sniff gently—you want the medicine to coat the inside of the nose, not shoot straight into the throat.
Start with proven basics that reduce daily burden—then add targeted therapies based on your pattern of symptoms.
Prescription treatments (what an ENT may recommend)
Intranasal corticosteroid sprays = first-line for many chronic inflammatory causes
Steroid nasal spray therapy is a cornerstone for chronic inflammatory conditions, including chronic rhinitis, CRS, and nasal polyps. EPOS 2020 and other clinical resources emphasize that improvement can build over days to a few weeks, not necessarily instantly. [1][2][3]
Many patients stop too early because it doesn’t feel like a decongestant. A realistic goal is steady improvement—better airflow at night, fewer flares, and improved smell over time.
Add-ons depending on symptoms
- Intranasal antihistamine sprays for mixed allergic/nonallergic symptoms [3]
- Anticholinergic sprays for prominent runny nose in selected patients [3]
Antibiotics—limited role in uncomplicated nasal congestion
For typical viral colds or uncomplicated rhinitis, antibiotics are generally not recommended. EPOS 2020 also emphasizes careful selection in suspected bacterial sinusitis and avoiding overuse. [1][3]
Oral steroids (short courses) — sometimes used, but not a long-term solution
Short courses may be used in specific scenarios (for example, significant inflammation or polyps), but they’re not a maintenance strategy and should be guided by a clinician. [1][2]
Emerging options for severe CRSwNP (biologic therapies)
For refractory, severe CRS with nasal polyps, biologic therapies (such as dupilumab or mepolizumab) are increasingly part of advanced care pathways in appropriate patients. [1][2]
Build anti-inflammatory control first; reserve antibiotics and oral steroids for carefully selected situations.
When structural problems need procedures or surgery
Signs you may need an ENT procedure
- Obstruction persists despite appropriate medical therapy
- There is significant septal deviation, valve collapse, large turbinates, or polyps [3]
In other words: if inflammation treatment is optimized and breathing still feels blocked, it’s time to re-check the anatomy.
Common procedures (patient-friendly overview)
- Septoplasty (to correct a deviated septum) [3]
- Turbinate reduction (to reduce airflow resistance from enlarged turbinates) [3]
- Polypectomy (remove polyps) [1][3]
- Balloon sinuplasty (selected cases of chronic sinus outflow obstruction) [1][3]
- Functional endoscopic sinus surgery (FESS) for refractory CRS/CRSwNP [1]
If ongoing symptoms suggest chronic rhinosinusitis (CRS), this overview of chronic sinusitis treatment can be helpful: https://sleepandsinuscenters.com/chronic-sinusitis-treatment
If optimized medical therapy isn’t enough, anatomy-focused procedures can restore airflow and improve quality of life.
Lifestyle tips to breathe better long-term (prevention + symptom control)
Allergen and irritant control (high-impact basics)
- Dust mite basics: mattress/pillow covers, hot-wash bedding, reduce carpet when possible
- Pet dander planning if sensitized
- Avoid smoke/vape exposure; minimize strong fragrances and harsh cleaning fumes [3]
Nasal hygiene routine (simple and sustainable)
- Many people use a saline rinse more often during flares and scale back when dryness is an issue. [1][3]
- If prescribed, consistent use of a steroid nasal spray is often more effective than intermittent use. [1][3]
Sleep-focused tips
- Side sleeping and gentle head-of-bed elevation may help some people when congestion worsens lying flat
- Addressing nasal blockage may reduce mouth breathing and snoring triggers [3]
Small, sustainable habits can meaningfully reduce day-to-day congestion and improve sleep.
FAQs (FAQPage)
Why can’t I breathe through my nose but I’m not “sick”?
Persistent trouble breathing through the nose without feeling ill is often related to chronic rhinitis, turbinate hypertrophy, a deviated septum, or nasal valve collapse. [3]
Do I need antibiotics for a stuffy nose or sinus symptoms?
Often, no—especially for viral colds or uncomplicated rhinitis. Antibiotics are typically reserved for appropriately selected cases, and overuse is discouraged in major guidelines. [1][3]
What’s the best first treatment for long-term nasal inflammation?
For many chronic inflammatory causes (including CRS and polyps), intranasal corticosteroid sprays are considered a key first-line treatment option. [1][2][3]
How do I know if I have nasal polyps?
Clues include chronic blockage and reduced smell. Diagnosis is confirmed by nasal exam and often endoscopy. [1][3]
When should I see an ENT for nasal obstruction?
Consider an ENT evaluation when symptoms persist for 12 weeks or more, are one-sided, include frequent nosebleeds, or do not improve with appropriate treatment. For acute symptoms, seek medical evaluation if they worsen—especially beyond about 10 days—or are accompanied by red flags.
Is it safe to use decongestant sprays every day?
Daily long-term use isn’t recommended due to the risk of rebound congestion from topical decongestant spray overuse (often after more than 3 consecutive days). [3]
Conclusion — A clear next step for readers
Trouble breathing through the nose usually comes down to either inflammation (often reversible) or structural narrowing (which may need targeted procedures). Saline rinses, trigger control, and anti-inflammatory nasal therapies can be helpful for many people, while persistent or one-sided obstruction often benefits from a more detailed evaluation.
If you’re dealing with ongoing nasal obstruction, our team can help you sort out the cause and review treatment options—from medical therapy to ENT procedures when appropriate. To get started, book an appointment at https://www.sleepandsinuscenters.com/.
A tailored plan that addresses both inflammation and anatomy offers the best chance for lasting relief.
Sources
1. EPOS 2020: European Position Paper on Rhinosinusitis and Nasal Polyps 2020 — https://www.rhinologyjournal.com/Documents/Supplements/supplement_29.pdf
2. A Comprehensive Review Exploring Allergic Rhinitis With Nasal Polyps (PMC, 2024) — https://pmc.ncbi.nlm.nih.gov/articles/PMC11130740/
3. Cleveland Clinic – Nasal Obstruction (2024) — https://my.clevelandclinic.org/health/symptoms/nasal-obstruction
Medical disclaimer
This article is for general education and is not a substitute for medical advice, diagnosis, or treatment. If you have severe symptoms or red flags (especially one-sided bleeding, facial/eye swelling, or confusion), seek urgent care.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.