Septoplasty Nose Splints: Benefits, Types, and Recovery Tips
If you are having or just had a septoplasty, it can be surprising to wake up feeling like there is something in your nose. That sensation is often due to nose splints or nasal packing placed at the end of surgery to support healing and reduce bleeding.
Good to know: splints or packing are common but not always required. Many surgeons now use options often better tolerated (absorbable nasal packing, silicone septal splints, or transseptal quilting sutures) rather than routine nonabsorbable packing for every patient. A meta-analysis found routine nonabsorbable packing after septoplasty is not superior to alternatives and may be associated with more discomfort, especially at removal (1).
If you are still exploring whether surgery is right for breathing problems, see an overview on deviated septum relief: https://sleepandsinuscenters.com/deviated-septum-relief
What Are Septoplasty Nose Splints (and How Are They Different From Nasal Packing)?
Both splints and packing can feel similar because each can create a congested, blocked sensation. A simple way to think about it: packing mainly provides gentle pressure for bleeding control, while splints mainly stabilize and separate healing surfaces. Your surgeon may use one, the other, or a combination.
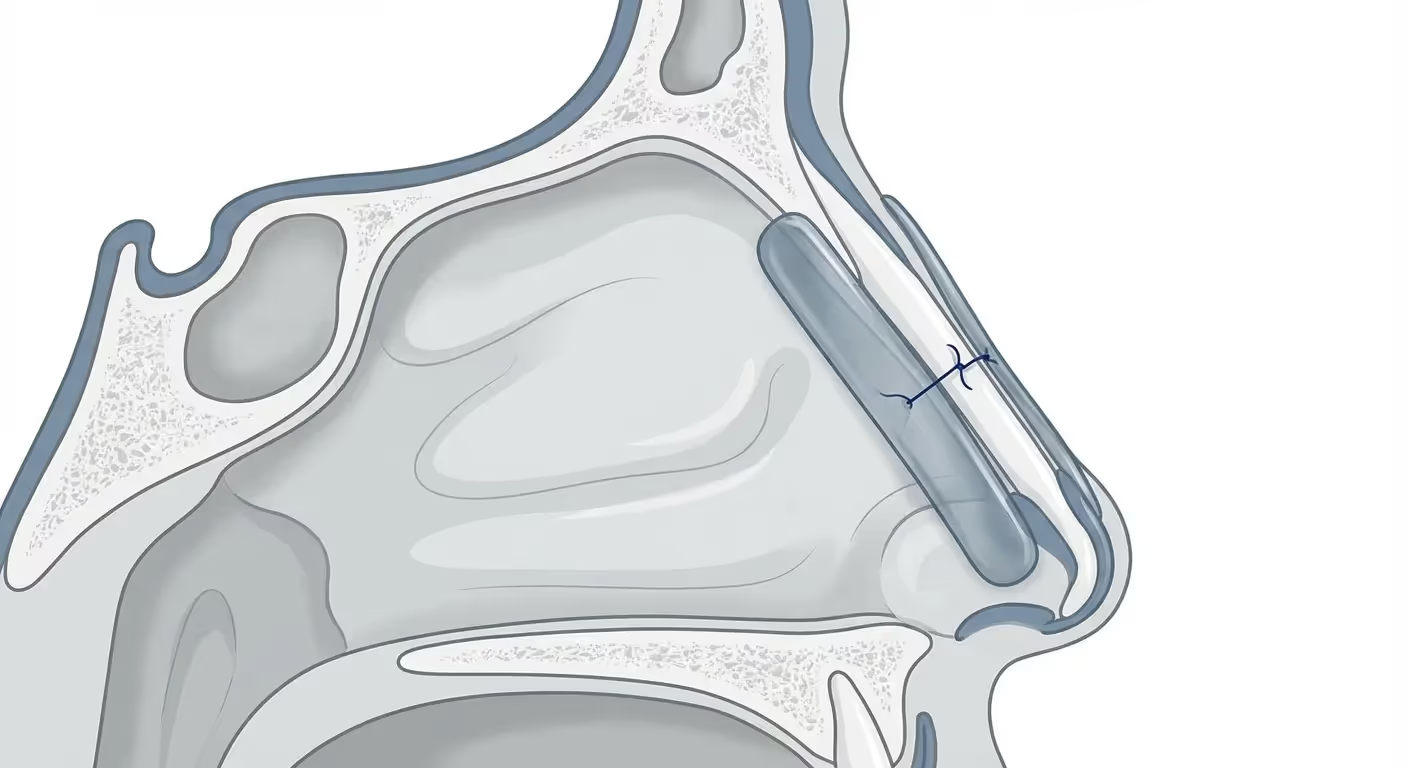
Septal splints: what they do
Thin supports placed along one or both sides of the septum, often secured with a small stitch. They stabilize the septum, reduce friction and trauma to healing tissues, and lower the chance of internal scar bands forming. Many ENT teams describe splints as a temporary internal cast.
Nasal packing: what it does
Material placed inside the nasal cavity to reduce bleeding through gentle pressure and to support tissues during early healing. Packing may be nonabsorbable (removed in the office) or absorbable (dissolves over time or is gently suctioned during follow-up). Absorbable options often feel less dramatic at removal.
Why surgeons choose one option over another
The decision depends on bleeding risk, how much structural support is needed, airway comfort, and surgeon experience. Evidence does not show routine nonabsorbable packing is superior after septoplasty (1). Comfort can vary by material.
Summary: think of packing as pressure for bleeding control and splints as structural support; your surgeon tailors the approach to your anatomy and risk profile.

Why Nose Splints Are Used After Septoplasty (Benefits for Healing)
Helps prevent septal hematoma
Supportive devices (splints, packing, or quilting sutures) reduce dead space where fluid could collect, lowering the risk of a blood collection under the septal lining.
Supports the septum as swelling settles
Early swelling is expected; splints provide gentle stabilization so the septum is less likely to shift. Patients often describe pressure and stuffiness during this phase.
Helps reduce internal scar bands
Splints can act as temporary spacers so nearby surfaces do not scar together and narrow airflow. See more on nasal synechiae: https://sleepandsinuscenters.com/blog/nasal-synechiae-after-surgery-causes-symptoms-and-treatment-options
Can reduce bleeding with improved comfort at removal
Modern absorbable packing materials and splints may control bleeding comparably to traditional packing, often with improved comfort, especially because some options avoid a single pull-out removal event (1-3).
Summary: splints, packing, and quilting sutures aim to prevent fluid pockets, stabilize tissues, and limit scar bands to support safer, more comfortable early healing.

Types of Septoplasty Nose Splints and Packs (Pros, Cons, and Who They Are For)
Surgeons may combine approaches, such as splints plus quilting sutures, depending on anatomy and bleeding risk.
Silicone septal splints (often nonabsorbable)
Nonabsorbable; sometimes include airway channels depending on model; typically removed in the office. Provide predictable support but can feel congesting until removed.
Splints with an airway channel
Nonabsorbable; airway channel present; in-office removal. May lessen the sensation of blockage, though channels can crust and feel dry without moisture care.
Absorbable synthetic polyurethane foam
Absorbable; no airway channel; dissolves over days to weeks with possible gentle suctioning of remnants. Studies suggest outcomes similar to nonabsorbable packing with less removal pain in some cohorts (2-3).
Chitosan-based absorbable packing
Absorbable; no airway channel; dissolves over time with potential suctioning of remnants. One randomized trial reported smaller early middle-ear pressure changes compared with silicone airway splints (5).
Traditional nonabsorbable packing
Nonabsorbable; no airway channel; in-office removal. Can feel tight with uncomfortable removal; not proven superior as a routine step (1).
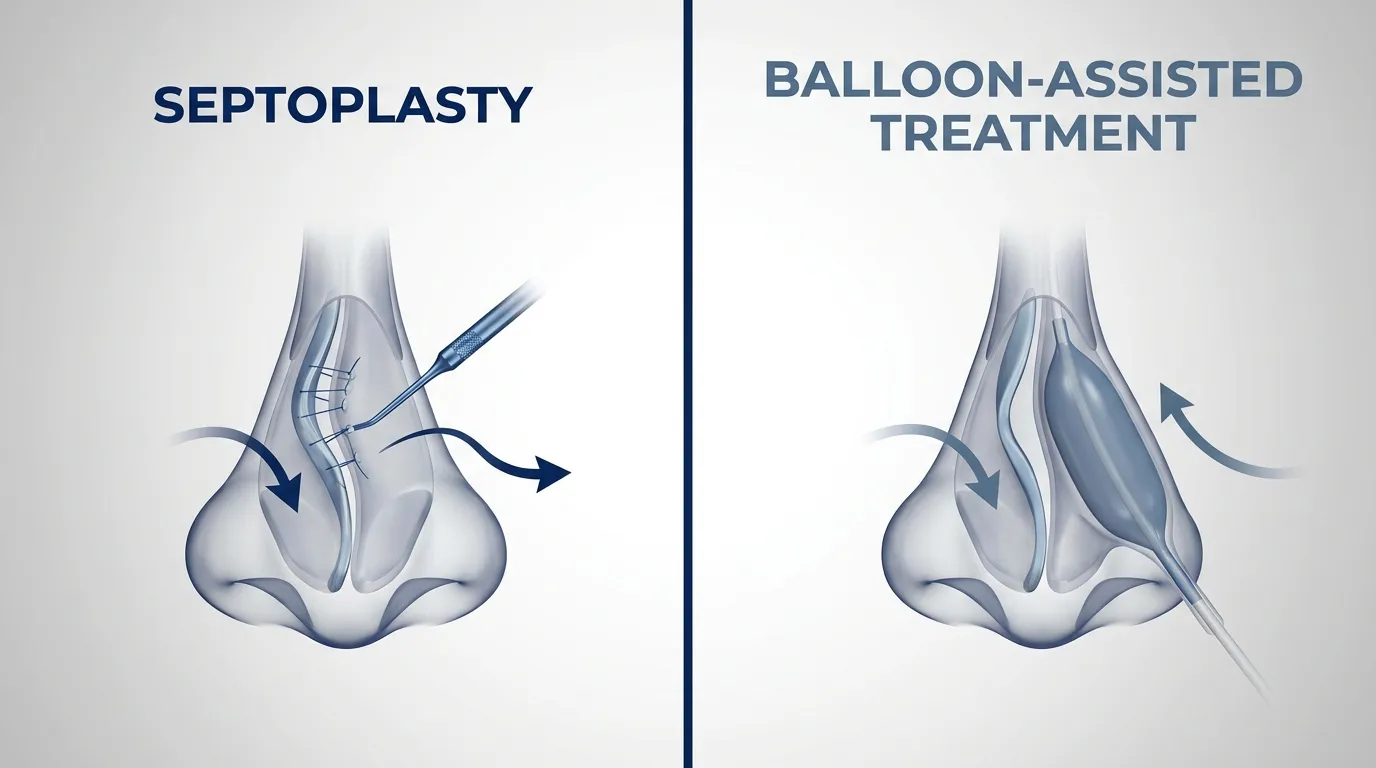
Transseptal quilting sutures
No packing to remove; used to close dead space and support healing; evidence-supported option that can avoid routine packing (1).
Summary: different materials balance support, bleeding control, airflow, and comfort; your surgeon selects the combination that fits your anatomy and risk factors.

What You May Feel With Splints In (Symptoms Patients Commonly Notice)
Normal sensations
Congestion or blockage, mild to moderate pressure, post-nasal drip or throat dryness from mouth breathing, temporary reduction in smell or taste, and mild blood-tinged mucus are common. One side can feel more blocked than the other due to asymmetric swelling or crusting.
Ear symptoms and why they happen
Swelling and pressure changes in the nose can affect the Eustachian tube and middle-ear pressure. Mild ear fullness or popping when swallowing is often temporary; some materials may be associated with smaller early pressure changes (5).
Red flags to report
Heavy bleeding that does not slow; fever, worsening facial pain, or foul smell; sudden worsening pain or new septal swelling; vision changes, severe headache, stiff neck, or significant breathing difficulty.
Summary: mild blockage, pressure, and ear popping are common early on; escalating pain, heavy bleeding, or new swelling warrant a prompt call to your care team.

How Long Do Septoplasty Splints Stay In?
Nonabsorbable splints are often removed around days 3 to 7, with timing individualized based on surgeon preference and the specifics of your procedure.
Absorbable packing dissolves over days to weeks, and remnants may be gently suctioned during follow-up instead of being pulled out. For a broader healing timeline, see septoplasty recovery week by week: https://sleepandsinuscenters.com/blog/septoplasty-recovery-week-by-week-complete-timeline
Summary: most nonabsorbable splints come out within a week; absorbable materials gradually break down and may be suctioned during follow-up.

Splint Removal: What to Expect (and How to Make It Easier)
Is removal painful?
Many describe removal as intense pressure or brief discomfort more than sharp pain. Absorbable options can reduce removal discomfort because there may not be a single traction-based event. Visits are usually quick, and many feel immediate relief afterward (2-3).
Tips before your appointment
Use saline sprays as directed to soften crusting; avoid blood-thinning medications unless approved; eat lightly if you feel faint with procedures; consider arranging a ride if you are anxious or lightheaded. Always follow your surgeon’s specific instructions.
Summary: removal is typically quick; softening crusts with saline and arranging support can make the visit smoother.
Septoplasty Recovery Tips (Day-by-Day Comfort and Better Healing)
First 24 to 72 hours
Rest, hydrate, and sleep with head elevated. Avoid nose blowing early and sneeze with your mouth open. Side-sleepers often do better propped up to avoid rolling onto the face.
Nose care routine
Use saline spray to keep the lining moist; start saline rinses when approved to clear mucus and crusting; consider a nighttime humidifier for dryness. Use ointments or gels only if specifically recommended. Gentle, frequent moisture beats aggressive cleaning.
Sleep tips
Elevate the head to reduce swelling. Hydration and humidification can ease mouth-breathing dryness. If you use CPAP, coordinate timing and settings with your ENT team.
Activity restrictions
Avoid heavy lifting or straining early and be cautious with heat if it triggers bleeding. Return-to-exercise timing varies; follow the plan provided. If activity causes throbbing or bleeding, scale back and call your surgeon if it persists.
Diet and lifestyle
Hydration and lower-salt choices may help swelling. Avoid smoking or vaping, which slow healing. Limit alcohol early due to swelling and bleeding risk.
Summary: gentle moisture, head elevation, and activity moderation are common comfort measures; let your surgeon’s plan guide your routine.
Treatments and Decision-Making: Which Option Is Best After Septoplasty?
Overall, modern research suggests absorbable packs and splints are at least as effective as nonabsorbable packing for bleeding control and hematoma prevention, often with improved comfort (1-3). Nonabsorbable packing is not proven superior as a routine step (1). If you are still deciding about surgery: https://sleepandsinuscenters.com/blog/is-septoplasty-right-for-your-deviated-septum
Questions to ask your surgeon
Will I have splints, packing, quilting sutures, or a combination; if packing is needed, is absorbable an option; will I be able to breathe through my nose with these in; how will you manage bleeding risk in my case.
Summary: there is no single best device for everyone; discuss materials and removal plans so expectations match your needs.
FAQs About Septoplasty Nose Splints
Can I breathe through my nose with splints in?
Sometimes partially, sometimes very little during the first few days when swelling is highest. Airway-channel splints may help some patients, though airflow can still feel limited.
Is it normal to have ear pressure after septoplasty?
Mild ear fullness or popping can occur temporarily due to Eustachian tube effects from swelling and pressure changes. Some materials may be linked to smaller early pressure changes (5).
What if a splint feels like it moved?
A shifting sensation can occur with swelling changes or crusting. Contact your surgical team for guidance rather than trying to reposition anything yourself.
Do splints prevent complications?
They reduce risks like septal hematoma or adhesions but do not eliminate risk. Good follow-up and aftercare also matter.
When can I return to work or school?
Many people return within about a week depending on job demands and recovery; your surgeon’s timeline is the best reference.
What is the difference between splints and stents?
Terms are sometimes used interchangeably. Generally, splints support the septum, while stents keep a passage open. In post-septoplasty discussions you may hear either term.
Summary: short-term stuffiness and ear pressure are common; when in doubt, ask your surgeon, especially if symptoms escalate or feel unusual.
When to Call Your ENT (Quick Safety Checklist)
Seek prompt guidance for persistent bright-red bleeding; fever above your team’s threshold; worsening severe pain, new swelling, or foul drainage; trouble breathing, chest pain, severe headache, or vision symptoms.
Summary: if symptoms escalate, do not wait; contact your care team for tailored guidance.
Conclusion
Whether you receive septoplasty nose splints, packing, quilting sutures, or a combination, these are temporary tools designed to support healing and reduce complications early in recovery. Today’s options, including absorbable materials, often improve comfort without sacrificing effectiveness (1-3). For questions or to schedule a visit: https://www.sleepandsinuscenters.com/
Summary: modern materials and techniques can make recovery smoother; your surgeon’s plan should reflect your anatomy, goals, and comfort.
Medical disclaimer: This article is for general education and is not a substitute for personalized medical advice. Always follow your surgeon’s specific post-operative instructions and contact your care team with concerns.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
1. Kim JS, Kwon SH. Is nonabsorbable nasal packing after septoplasty essential? A meta-analysis. Laryngoscope. 2017;127(5). https://pubmed.ncbi.nlm.nih.gov/27900768/
2. An JS, et al. Comparison of Outcomes After Septoplasty With Non-Absorbable or Biodegradable Synthetic Polyurethane Foam Nasal Packing. J Rhinol. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC11524360/
3. Yilmaz MS, et al. An evaluation of biodegradable synthetic polyurethane foam in patients following septoplasty. Otolaryngol Head Neck Surg. 2013. https://pubmed.ncbi.nlm.nih.gov/23112275/
5. Elden H, et al. Effect of Chitosan-Based Biodegradable Nasal Packs on Eustachian Dysfunction after Septoplasty. 2025 RCT. https://pmc.ncbi.nlm.nih.gov/articles/PMC12422843/
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.