

Best Nasal Sprays for Acute Bacterial Rhinosinusitis: Top Options and How to Use
When you feel stuffed up, pressured, and miserable, it’s natural to search for the “best nasal spray for bacterial sinus infection.” The key is recognizing what nasal sprays can do well—reduce swelling, improve drainage, and ease congestion—and what they typically cannot do alone: cure a true bacterial infection deep in the sinuses. Sprays are most useful for symptom relief and supportive care, alongside clinician-directed treatment when needed.
Medical disclaimer: This article is for general education and does not replace medical advice. If you have severe symptoms, red flags, or persistent/worsening illness, seek medical care.
Quick Answer (Key Takeaways)
- Acute bacterial rhinosinusitis (ABRS) is primarily treated with oral antibiotics when truly bacterial, not with over-the-counter “antibiotic nasal sprays.” Guideline-based diagnosis and antibiotic stewardship matter. (AAFP, AAO-HNS, IDSA)
- The most helpful nasal sprays for symptom relief during bacterial sinusitis are usually: saline spray or irrigation to thin and clear mucus and support drainage; intranasal corticosteroid sprays (such as fluticasone or mometasone) to reduce inflammation and congestion.
- In select chronic or refractory cases, ENT specialists may use prescription, culture-directed topical antibiotic irrigations delivered by high-volume rinse methods (this is not the same as a standard OTC spray bottle).
- Decongestant sprays can open the nose quickly, but overuse may cause rebound congestion (rhinitis medicamentosa). Use only as directed, and generally avoid using decongestant sprays for more than 3 days unless a clinician advises otherwise. For details, see: https://sleepandsinuscenters.com/blog/afrin-rebound-how-long-does-nasal-congestion-last-after-use
- Antibiotics may still be needed when symptoms persist, worsen, or are severe in a way that supports ABRS. For background: https://sleepandsinuscenters.com/blog/do-i-always-need-antibiotics-for-a-sinus-infection
• In short: saline plus a steroid spray often provides the best symptom relief, while antibiotics are considered when ABRS criteria are met.
What Is a Bacterial Sinus Infection (and Why Sprays Alone Don’t “Cure” It)?
Sinusitis occurs when the sinus lining becomes inflamed and swollen, trapping mucus and causing pressure. Many episodes begin as viral colds; some progress to acute bacterial rhinosinusitis.
Typical pattern: you catch a cold → the nasal passages and sinus openings swell → mucus thickens and gets trapped → pressure builds → symptoms linger or worsen. Sprays help reduce swelling and improve drainage, which is why they’re valuable—even when antibiotics are needed.
Acute rhinosinusitis vs. chronic rhinosinusitis (CRS)
- Acute rhinosinusitis: symptoms typically last less than 4 weeks.
- Chronic rhinosinusitis (CRS): symptoms persist more than 12 weeks and often involve ongoing inflammation, allergies, nasal polyps, or structural blockage. CRS often needs longer-term management and sometimes ENT evaluation.
Why most standard sprays cannot fully treat deep sinus infection: most sprays coat the nasal passages and may not deliver medication uniformly into the deeper sinus cavities where infection and trapped mucus can reside. When bacterial sinusitis is strongly suspected, clinicians consider systemic (oral) antibiotics because they reach the sinus tissues through the bloodstream. Sprays remain essential to reduce swelling and improve drainage, which supports recovery and comfort.
• Bottom line: sprays help the nose work better and ease symptoms, but they are usually not definitive treatment for ABRS by themselves.
Symptoms That Suggest Sinusitis (and When It Might Be Bacterial)
Common sinus infection symptoms
- Facial pressure or fullness
- Nasal congestion or blocked nose
- Thick nasal discharge or post-nasal drip (often drives cough, particularly at night)
- Reduced sense of smell
- Headache or dental pain
Clues that raise suspicion for acute bacterial rhinosinusitis (vs viral). Color alone isn’t enough. Guideline-based “bacterial” patterns include:
- Persistent symptoms that do not improve for about 10 days or longer
- “Double-worsening” (you start to improve, then symptoms worsen again)
- Severe symptoms (such as significant fever with purulent discharge and facial pain)
For a deeper comparison, see: https://sleepandsinuscenters.com/blog/viral-vs-bacterial-sinus-infections-key-differences
Red flags—seek urgent medical care
- Eye swelling or vision changes
- Severe headache, stiff neck, confusion
- High fever, significant facial swelling
- Immune compromise or serious underlying illness
• If symptoms are protracted, severe, or worsening—especially with red flags—seek prompt evaluation.
Causes and Risk Factors (Why You Got It)
Common triggers
- A viral upper respiratory infection that leads to secondary bacterial infection
- Allergies that inflame and block nasal passages
- Structural issues (deviated septum, nasal polyps)
- Smoke/irritants and poor air quality
Why inflammation matters: inflammation narrows drainage pathways. When mucus cannot drain, it thickens and stagnates—leading to congestion, pressure, and sometimes infection. Individual anatomy, allergies, and baseline inflammation explain why some people develop longer-lasting sinus problems after a common cold.
• Managing inflammation and improving drainage paths are central to feeling better.
Treatments That Address the Infection (Not Just Symptoms)
When oral antibiotics are considered: not every sinus infection needs antibiotics. When symptoms match bacterial criteria, clinicians may recommend antibiotics for ABRS based on guidelines (AAFP, AAO-HNS, IDSA). If you’re unsure whether antibiotics are necessary, this overview can help: https://sleepandsinuscenters.com/blog/do-i-always-need-antibiotics-for-a-sinus-infection
Symptom control that helps you breathe while you heal
- Saline irrigation
- Intranasal corticosteroid sprays
These therapies reduce swelling and help move mucus out more effectively. Many patients describe the goal as “getting things moving again”—less blockage, better drainage, and less pressure.
• Antibiotics treat confirmed bacterial infection; saline and steroid sprays support drainage and day-to-day comfort.
Best Nasal Spray Options for a Bacterial Sinus Infection (Adjunctive Relief)
Important framing: The best nasal sprays for symptom relief during bacterial sinusitis are those that improve drainage and reduce inflammation; they do not replace clinician-directed treatment when ABRS is present.
Option 1 — Saline Spray or Irrigation (Best first step for most people)
- What it helps: loosens thick mucus, clears irritants/allergens, supports nasal hygiene and drainage
- Who it’s best for: most people, including many who cannot use medicated sprays
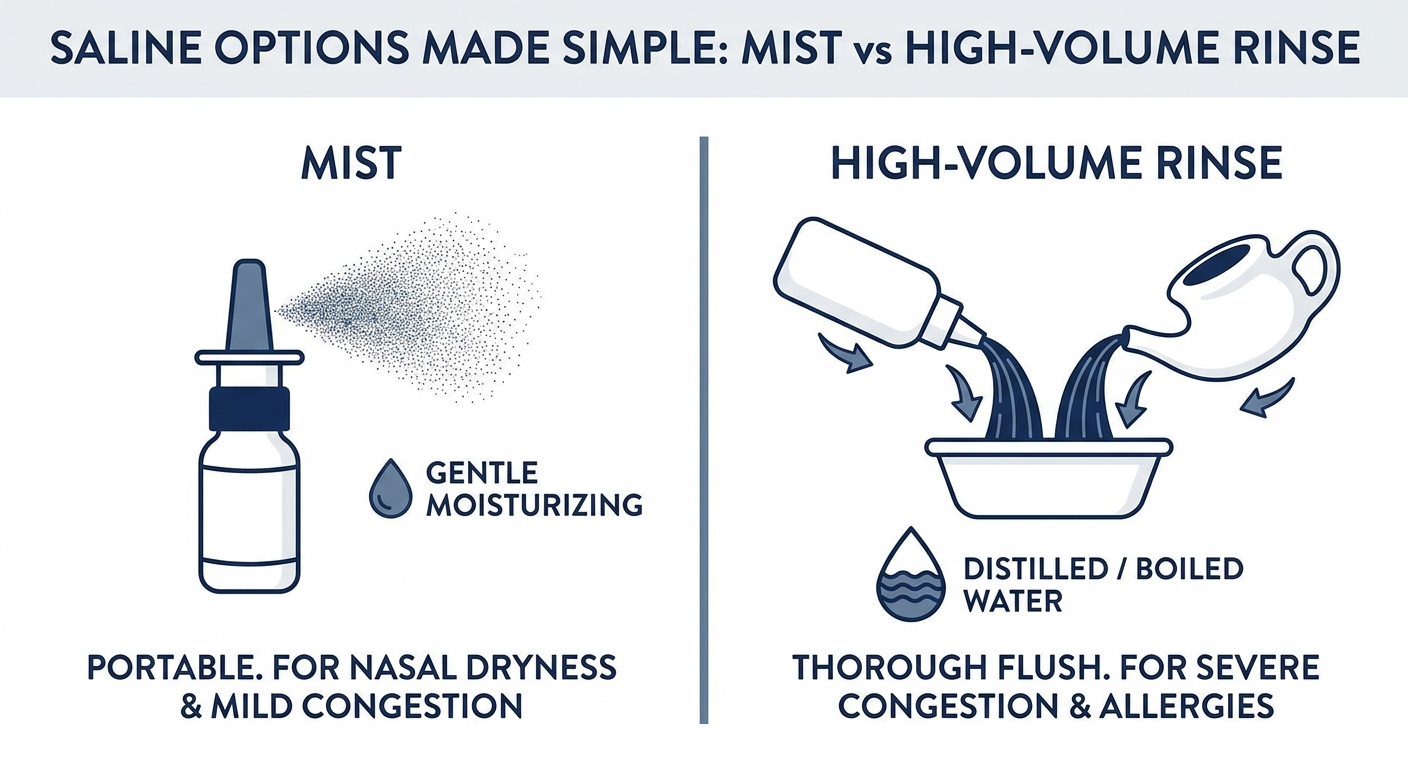
- Product forms: gentle saline mist sprays (easy, portable); high-volume irrigation (squeeze bottle or neti pot) that can flush more thoroughly
- Safety reminder: For any rinse, use distilled or sterile water, or water that has been previously boiled and cooled.

Option 2 — Intranasal Corticosteroid Sprays (Best for swelling and inflammation)
- Examples: fluticasone, mometasone, triamcinolone, budesonide (OTC or prescription varies)
- What it helps: reduces inflammation to improve congestion and drainage
- Best for: significant congestion, allergy history, recurrent sinusitis, and chronic rhinosinusitis symptoms

Option 3 — Decongestant Nasal Sprays (Use sparingly)
- Examples: oxymetazoline (Afrin), xylometazoline (varies by country)
- What it helps: rapidly shrinks swollen nasal tissue to open airflow
- Key caution: Use only as directed, and generally avoid using decongestant sprays for more than 3 days unless a clinician advises otherwise. Learn more: https://sleepandsinuscenters.com/blog/afrin-rebound-how-long-does-nasal-congestion-last-after-use
- Who should be cautious: People with certain cardiovascular conditions or on specific medications should speak with a clinician or pharmacist before use.
Option 4 — Antihistamine Nasal Sprays (If allergies are a driver)
- Example: azelastine (often prescription)
- What it helps: sneezing, itching, runny nose; may reduce post-nasal drip when allergies contribute
- What it doesn’t do: treat the infection itself—this is for allergy overlap
Special mention — XHANCE for Chronic Rhinosinusitis
XHANCE is a prescription fluticasone product with an exhalation delivery system designed to deliver medication deeper into the nasal cavity. It is used for certain chronic rhinosinusitis indications (with or without nasal polyps) and is not an antibiotic.
What about “antibiotic nasal sprays”?
There is no commonly used FDA-approved antibiotic nasal spray for routine acute bacterial sinusitis treatment. Be cautious about OTC products marketed with “antibiotic-like” claims. When topical antibiotics are used, it’s typically in specialized situations with high-volume irrigations under ENT supervision.
• For symptom relief, saline and steroid sprays are top choices; antibiotics are considered separately when ABRS criteria are met.
Prescription Topical Antibiotics: When ENT Doctors May Use Them (Advanced/Chronic Cases)
Culture-directed topical antibiotic irrigations (not a typical spray bottle). In select patients with recalcitrant or chronic rhinosinusitis, an ENT may use prescription, culture-directed topical antibiotic irrigations that are:
- Chosen based on identified bacteria
- Delivered via high-volume irrigation or, in some settings, nebulized methods
- Often compounded and monitored
Mupirocin (Bactroban) nasal ointment—what it is actually for: mupirocin nasal products are used for certain nasal vestibule infections or Staphylococcus aureus colonization; they are not designed to treat deep sinus cavities.
Why you shouldn’t DIY topical antibiotics in rinses: mixing antibiotics into home rinses without guidance can increase risks such as irritation, contamination, incorrect dosing, and antibiotic resistance.
• Topical antibiotics for sinus care are a specialist-directed option for select chronic or refractory cases, not a first-line therapy for routine ABRS.
How to Use Nasal Sprays Correctly
Before you spray: clear the path
- Gently blow your nose, or use saline first.
- Many people do best with rinse then spray, especially before steroid sprays, so medication contacts the lining better: https://sleepandsinuscenters.com/blog/rinse-then-spray-correct-order-for-effective-cleaning
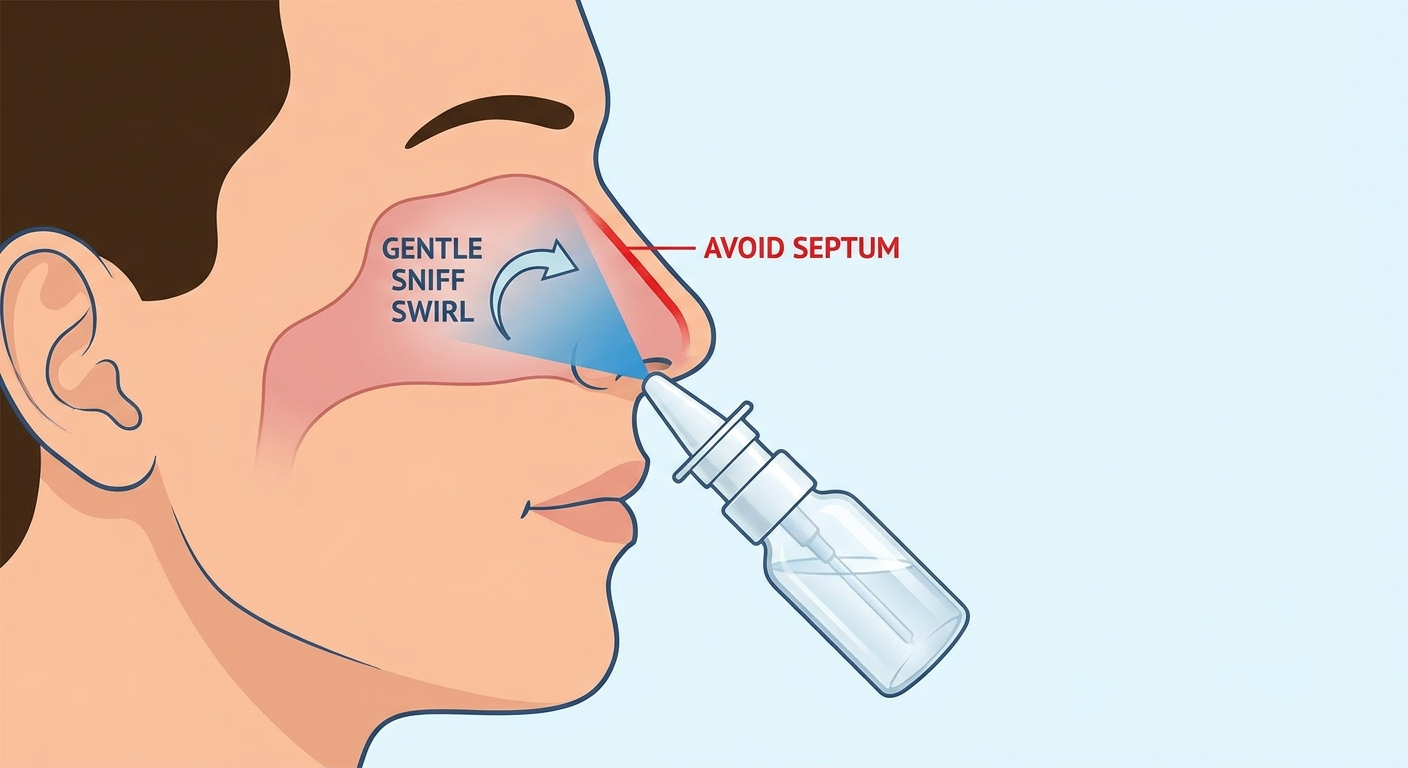
Proper spray technique (especially for steroid sprays)
- Aim the nozzle slightly outward, away from the septum (the middle wall)
- Use a light sniff—don’t inhale forcefully
- Keep your head neutral (avoid dramatic tilt back unless directed)
- Quick tip: If you taste medicine in your throat, you may be sniffing too hard.

Sample daily routine (simple and realistic)
- Morning: saline rinse → steroid spray
- Midday (optional): saline mist
- Night: steroid spray if directed twice daily, plus bedroom humidification if air is dry
How long until it works?
- Saline: immediate clearing (often temporary but helpful)
- Decongestant spray: minutes
- Steroid sprays: gradual—often several days, up to about 2 weeks for best effect
• Rinse first, spray second, and use gentle technique so medicine reaches the right place.
Safety, Side Effects, and Who Should Be Cautious
Common side effects by spray type
- Saline: mild irritation or dryness (hypertonic saline may sting)
- Steroid sprays: dryness, irritation, occasional nosebleeds—often improved by aiming away from the septum
- Decongestants: rebound congestion if overused; follow label directions
Pregnancy, kids, and chronic conditions: the safest choice varies by person. Check with your obstetrician, pediatrician, or clinician, especially for medicated sprays.
When sprays might make symptoms worse: stop and seek guidance if you develop frequent nosebleeds, worsening pain or pressure, fever, or symptoms that don’t improve as expected.
• Use sprays as directed, and involve your clinician if symptoms persist, worsen, or raise safety concerns.
Lifestyle and Home Tips That Support Recovery
- Hydration and humidification: help keep mucus thinner
- Warm showers or steam: can soothe and loosen mucus (comfort measure, not a bacteria-killer)
- Sleep positioning: slight head elevation may reduce congestion and post-nasal drip
- Reduce triggers: avoid smoke, manage allergies, and monitor indoor air quality
• Simple daily habits—hydration, humidity, and trigger control—can make sprays work better.
When to See a Doctor (or an ENT)
See a clinician if: symptoms last more than 10 days, worsen after initial improvement, or become severe.
Consider ENT evaluation if: frequent or recurrent infections; symptoms persist despite appropriate treatment; concern for chronic rhinosinusitis, nasal polyps, or structural blockage.
If you are in Georgia and symptoms keep coming back, Sleep and Sinus Centers of Georgia can help you determine whether you are dealing with recurring acute infections, allergies, or chronic sinus inflammation. Book an appointment: https://www.sleepandsinuscenters.com/
• Persistent, severe, or recurrent symptoms warrant professional evaluation—especially to assess for CRS or structural issues.
FAQs
What is the best nasal spray for bacterial sinus infection? For most people, the most helpful approach for symptom relief is saline irrigation plus an intranasal corticosteroid spray to reduce swelling and improve drainage. Antibiotics may still be needed when ABRS criteria are met.
Is there an antibiotic nasal spray for sinus infections? Not for routine acute bacterial sinusitis. Topical antibiotics are mainly used as prescription, culture-directed irrigations under ENT care for chronic or refractory cases.
Should I use saline or steroid spray first? Typically, saline rinse first, then steroid spray (“rinse then spray”) so the medication better contacts the nasal lining: https://sleepandsinuscenters.com/blog/rinse-then-spray-correct-order-for-effective-cleaning
Can I use Afrin/oxymetazoline for a sinus infection? It can help briefly, but use only as directed, and generally avoid more than 3 days unless a clinician advises otherwise: https://sleepandsinuscenters.com/blog/afrin-rebound-how-long-does-nasal-congestion-last-after-use
What if I have thick green mucus—does that mean bacterial? Not necessarily. Mucus color alone does not confirm a bacterial infection; duration, severity, and pattern matter more.
Can mupirocin treat a sinus infection? Mupirocin nasal products are intended for certain nasal vestibule infections or Staphylococcus aureus colonization, not for medicating the deep sinus cavities.
Conclusion
If you are searching for the best nasal spray for a bacterial sinus infection, the most evidence-supported “top picks” for symptom relief are saline irrigation and an intranasal corticosteroid—because they reduce congestion and inflammation and help the sinuses drain. When an infection is truly bacterial and meets guideline-based criteria, oral antibiotics may be appropriate. If symptoms are severe, lingering, or repeatedly returning, consider a comprehensive evaluation—especially to rule out chronic rhinosinusitis or ongoing triggers. Sleep and Sinus Centers of Georgia can help you find the right next step: https://www.sleepandsinuscenters.com/
Sources
1. American Academy of Family Physicians (AAFP) — Adult Sinusitis: https://www.aafp.org/family-physician/patient-care/clinical-recommendations/all-clinical-recommendations/adult-sinusitis.html
2. Infectious Diseases Society of America (IDSA) — Acute Bacterial Rhinosinusitis Guideline (2012): https://academic.oup.com/cid/article/54/8/e72/455098
3. American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) — Adult Sinusitis Guideline: https://www.entnet.org/resource/clinical-practice-guideline-adult-sinusitis/
4. Topical therapies/antibiotics in chronic rhinosinusitis (review): https://pmc.ncbi.nlm.nih.gov/articles/PMC5108841/
5. Mayo Clinic — Mupirocin (nasal): https://www.mayoclinic.org/drugs-supplements/mupirocin-nasal-route/description/drg-20064917
6. XHANCE — Product information: https://www.xhance.com/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.






