Maxillary Sinusitis: Symptoms, Causes, and Effective Treatments
If you’ve ever felt intense pressure in your cheeks, stubborn congestion, or even upper tooth pain that doesn’t quite feel “dental,” the maxillary sinuses may be involved. Maxillary sinusitis is inflammation (and sometimes infection) of the largest sinuses—located in your cheekbones—and it affects millions each year. It can be viral, bacterial, allergic, dental (odontogenic), or mixed in origin. When these sinuses swell and can’t drain well, symptoms like facial pressure, thick mucus, and fatigue can interfere with sleep, work, and everyday life. (See [1][2])
In this guide, you’ll learn the most common symptoms, the causes (including overlooked dental triggers), how clinicians typically diagnose it, and a “treatment ladder” that ranges from supportive home care to in-office procedures. Common triggers include viral illness, allergies, and dental issues. (See [1][2])

What Is Maxillary Sinusitis?
Maxillary sinusitis is inflammation in the maxillary sinuses—the air-filled spaces in your cheekbones. Sometimes that inflammation is driven by a virus or allergies; other times, bacteria are involved. In all cases, the “mechanical problem” is similar: swollen tissue plus thicker mucus can block drainage, which increases pressure and keeps irritation going. (See [1][2])
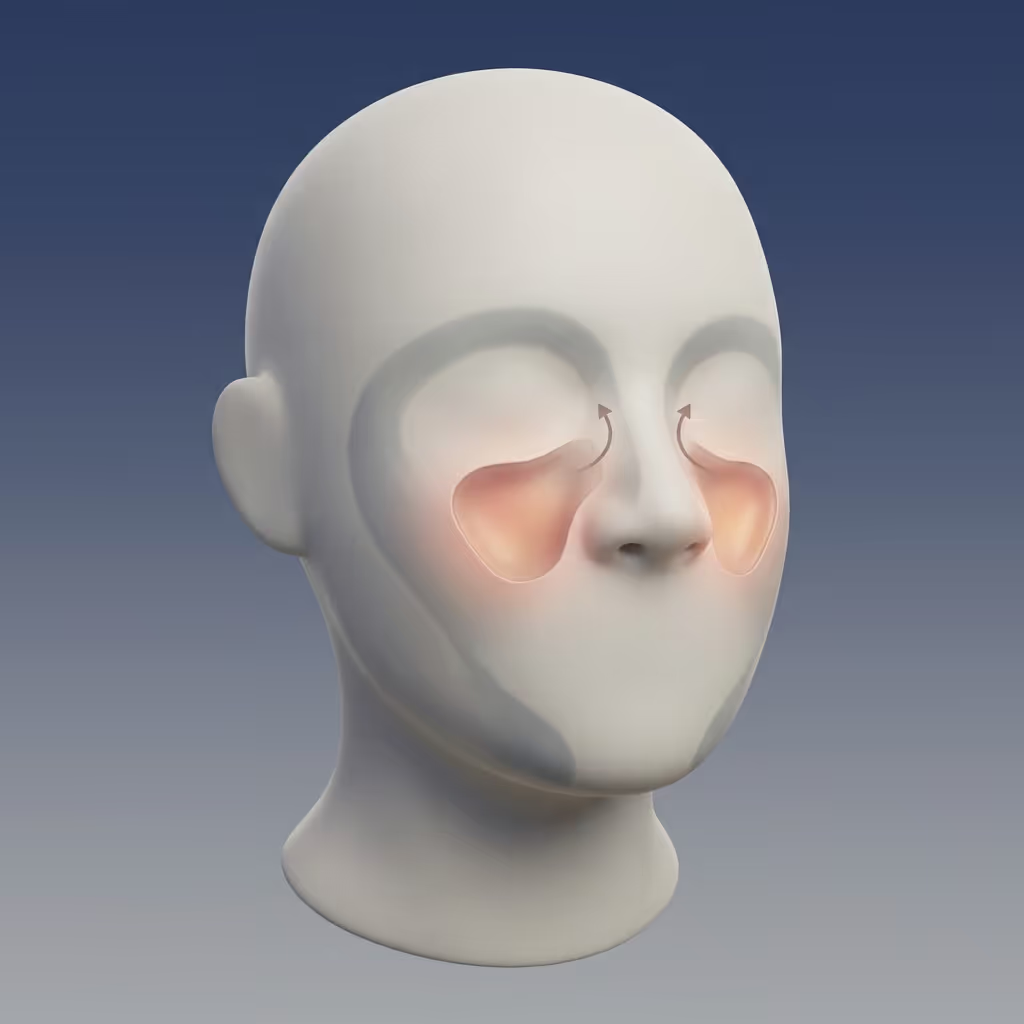
Where are the maxillary sinuses?
Your maxillary sinuses sit behind your cheeks and above the upper teeth, close to the roots of your upper molars. That anatomy matters: swelling or pressure in these sinuses can feel like jaw pressure or tooth pain—even when the teeth are healthy. (See [2][6])
A helpful way to picture it: the maxillary sinus is like a room with a narrow doorway (the drainage pathway). When the doorway swells partially shut, normal mucus can’t exit efficiently—so pressure and symptoms build.
Acute vs. chronic maxillary sinusitis (quick definitions)
If symptoms are persistent or frequently return, it often signals the need for a deeper evaluation of inflammation, drainage, anatomy, or possible dental sources. (See [2])
In short: maxillary sinusitis is a drainage problem driven by inflammation from viral, bacterial, allergic, or dental causes.

Maxillary Sinusitis Symptoms (What Patients Usually Notice)
Symptoms often come in clusters. Many people notice they’re more uncomfortable in the morning (after nighttime mucus pooling) or when bending forward (which can increase pressure sensations). The combination of location (cheeks/upper teeth) and drainage changes is one reason maxillary sinusitis can be so disruptive. (See [1][2])
Classic symptoms
Many people with maxillary sinusitis symptoms describe:
These patterns are common across sinusitis types, especially when swelling blocks normal drainage. (See [1][2][4])
A common patient description is: “It feels like my cheeks are heavy or full, like there’s pressure behind them.” Clinicians hear variations of this often, particularly during a cold or allergy flare.
For a broader overview, see our guide to the symptoms of sinus problems: https://sleepandsinuscenters.com/symptoms-of-sinus-problems
Symptoms that can mimic dental problems
Because the maxillary sinuses sit so close to the upper teeth, sinus inflammation may feel like:
When symptoms are mainly on one side, clinicians often consider localized causes—one of the most important being a dental source. (See [3][6])
A practical example: if your “toothache” worsens when you bend forward or improves when congestion improves, clinicians may think about sinus pressure as a contributor (even if you still need a dental exam to be sure).
Related reading: Can sinus problems cause tooth pain? https://sleepandsinuscenters.com/blog/can-sinus-problems-cause-tooth-pain
Other possible symptoms
Other symptoms can include:
These can happen with broader nasal inflammation and drainage changes. (See [2])
Bottom line: cheek pressure plus congestion and thick drainage—often worse when bending forward—are hallmark clues.

Causes of Maxillary Sinusitis (Infection, Allergies, and Dental Triggers)
Maxillary sinusitis usually has a “trigger” (like a cold, allergies, or a dental issue) and a “traffic jam” effect afterward: swollen lining and mucus lead to poor drainage, which prolongs symptoms. (See [2][4])
Viral upper respiratory infections (most common starting point)
Many cases begin after a cold or flu. Viral inflammation can swell the lining of the nose and sinuses, narrowing the drainage pathways and trapping mucus. (See [2][4])
In other words, the virus doesn’t have to “invade” the sinus itself for you to feel sinus pressure—nasal swelling alone can be enough to block normal flow.
Bacterial infection (when symptoms persist or worsen)
A maxillary sinus infection caused by bacteria is more likely when symptoms don’t improve as expected, last longer than typical viral illness, or worsen after initially improving. Clinicians often use the symptom timeline and severity to decide whether bacterial infection is likely. (See [2][4])
A clinician might put it like this: “The calendar matters.” Duration and symptom pattern often guide whether antibiotics are considered. To support antibiotic stewardship, antibiotics are generally reserved for cases with clear signs of bacterial infection in line with clinical guidelines. (See [2][4])
Allergies and chronic inflammation
Seasonal or year-round allergies can inflame nasal tissue, increase mucus, and contribute to drainage blockage—setting the stage for repeated sinus flare-ups. (See [1][2])
Some people notice a consistent seasonal pattern (for example, symptoms that reliably appear during peak pollen months), which can be a clue that inflammation—not just infection—is driving the cycle.
Odontogenic (dental) sinusitis — a major and often missed cause
Odontogenic sinusitis means sinusitis that starts from a dental problem, usually involving upper molars or dental procedures close to the maxillary sinus floor. Common triggers include:
A key point: odontogenic causes may account for ~10–40% of cases—especially when symptoms are unilateral (one-sided). (See [3][6])
This is why ENT clinicians often ask very specific questions about dental history when symptoms are stronger on one side or seem to follow a procedure. (See [3][6])
Structural or drainage issues that increase risk
Some people are more prone to recurring symptoms because of physical blockage or narrowed drainage pathways, such as:
These issues can make inflammation “stickier” and more likely to return. (See [2])
In short: identify the trigger and clear the “traffic jam” to break the cycle.

How Maxillary Sinusitis Is Diagnosed
Many cases can be evaluated based on symptoms and exam alone—especially when the pattern fits a straightforward, short-term episode. When symptoms linger, recur, or look one-sided, clinicians often widen the workup to avoid missing underlying causes. (See [1][2][6])
Medical history + symptom timeline (what your clinician asks)
Diagnosis often starts with details that may seem simple but are extremely useful:
This history helps narrow down likely causes and next steps. (See [1][2])
Physical exam (nose/throat/face)
A typical exam may include looking for:
These findings help confirm patterns consistent with sinus inflammation. (See [2])
Imaging (when it’s needed)
Not everyone needs imaging. However, a sinus CT scan may be used when symptoms are chronic, recurrent, unusually severe, or when clinicians suspect a complication, a structural blockage, or a dental source. CT imaging is especially helpful for mapping anatomy and identifying areas of trapped inflammation. (See [1][6])
You can think of CT as a “road map” for the sinuses: it helps clinicians see where swelling or blockage is occurring and whether anatomy may be contributing. (See [6])
Learn more: what a sinus CT scan shows and how it helps diagnose sinus issues https://sleepandsinuscenters.com/blog/sinus-ct-scan-what-it-shows-and-how-it-helps-diagnose-sinus-issues
When dental evaluation matters
A dental evaluation becomes especially important when red flags suggest a tooth-related source, such as:
In these cases, treating the sinus without addressing the tooth source may lead to incomplete improvement. (See [3][6])
Takeaway: the story, the side, and (when needed) a CT “map” point to the cause and guide treatment.
Maxillary Sinusitis Treatments (From Home Care to Procedures)
Treatment is usually tailored to the cause (viral vs. bacterial vs. allergy vs. dental), the duration, and how much blockage is present. Below is an educational overview of options clinicians commonly consider for maxillary sinusitis treatment. (See [2][4])
A simple way to think about the “treatment ladder”
Many treatment plans move from least invasive to more targeted interventions. The goal is usually to (1) reduce inflammation, (2) improve drainage, and (3) address any underlying trigger—especially allergies or dental sources when present. (See [2][3][4])
First-line at-home and supportive care
Supportive care is often used to promote comfort and drainage, such as:
These approaches are commonly recommended as part of conservative care. (See [2][4])
Example: many patients find that a consistent saline rinse routine during a flare helps reduce the “stuck” feeling of thick mucus, even if it doesn’t instantly eliminate pressure. (See [2][4])
Over-the-counter symptom relief (use carefully)
Depending on health history and medication compatibility, people may consider OTC options for discomfort and congestion. Clinicians often caution that:
(See [2])
Prescription options (when symptoms suggest more than a simple cold)
If symptoms and timeline suggest bacterial infection or significant inflammation, clinicians may consider:
To support antibiotic stewardship, prescription antibiotics are generally reserved for cases with clear signs of bacterial infection and not used routinely for viral illness. (See [2][4])
Treating odontogenic sinusitis (you often need both ENT + dental care)
With odontogenic sinusitis, the “source problem” often needs attention first (or in parallel):
This combined approach matters because symptoms often persist if the dental trigger remains untreated. (See [3][6])
In practice, that can mean coordinating timelines so dental infection control and sinus drainage improvement happen in a logical sequence. (See [3][6])
Office-based or procedural treatments for persistent cases
When symptoms persist despite appropriate medical therapy and evaluation, selected patients may be candidates for procedures designed to improve drainage. One option is balloon sinuplasty, a minimally invasive way to open blocked drainage pathways in carefully selected cases. Balloon sinuplasty is not appropriate for everyone; candidacy depends on individual assessment. (See [1][5])
More information: balloon sinuplasty https://www.sleepandsinuscenters.com/balloon-sinuplasty
Surgery for chronic or complicated disease
For chronic disease, severe blockage, polyps, or anatomy issues contributing to repeated flare-ups, clinicians may recommend endoscopic sinus surgery. The goal is to improve ventilation and drainage and reduce recurrence. (See [2][6])
Takeaway: start conservative, treat the cause, and reserve antibiotics and procedures for the right scenarios.

Lifestyle Tips to Prevent Recurrence (Patient-Friendly, Practical)
Reduce triggers
(Allergies and irritants can drive ongoing inflammation. See [2].)
Support sinus drainage and mucus health
(See [2][4])
Dental prevention (often overlooked)
This is especially relevant because dental sources are common in unilateral cases. (See [3][6])
Small, consistent habits can lower flare-ups and keep drainage moving.
When to See a Doctor (and When It’s Urgent)
Consider medical evaluation if:
(See [2])
If you’re unsure, it’s reasonable to check in sooner when symptoms are mostly one-sided or tied to tooth pain—those patterns often deserve a closer look. (See [3][6])
Seek urgent care for red flags
(See [2])
If symptoms linger, worsen, or are one-sided—especially after dental work—get checked.
FAQs About Maxillary Sinusitis
Why does maxillary sinusitis cause tooth pain?
Because the maxillary sinuses sit close to the roots of the upper teeth, inflammation and pressure can refer pain to the teeth and jaw. (See [6])
Is green mucus always a bacterial infection?
Not always. Mucus color can change with inflammation from viral illness as well; the overall pattern, timeline, and severity are more informative. (See [2])
How do I know if my sinus infection is from a tooth?
Clues include one-sided symptoms, upper tooth pressure, a history of recent dental work, or persistent symptoms that don’t respond as expected. (See [3][6])
What’s the fastest way to feel better?
Relief often comes from supportive care (hydration, saline rinses) and targeted treatment when appropriate. When symptoms persist or recur, evaluation for allergies, anatomy, or dental sources can be important. (See [2][4])
When is balloon sinuplasty considered?
Balloon sinuplasty is typically considered for ongoing blockage or chronic symptoms that don’t respond to medical therapy, and patient selection matters. (See [1][5])
Conclusion (Recap + Next Step)
Maxillary sinusitis commonly causes cheek pressure, congestion, and thick drainage—and it can sometimes mimic dental pain. Causes range from viral illness and allergies to bacterial infection and dental triggers like odontogenic sinusitis. Diagnosis often relies on symptom history, an exam, and—in selected cases—imaging such as a sinus CT scan. Treatment typically progresses from supportive care to medications, and for persistent blockage, procedures may be considered.
If symptoms are persistent, recurring, or mostly one-sided—especially after dental work—an evaluation can help clarify the cause and map out options. To explore next steps, browse our symptom resources or book an appointment with Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
References
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.