Lupus and Chronic Sinus Problems: Symptoms, Causes, and Treatment Options
Introduction — Why sinus problems are common in lupus
Systemic Lupus Erythematosus (SLE), often called lupus, is an autoimmune condition that can affect many parts of the body—including the nose and sinuses. For some people, this autoimmune activity manifests as persistent nasal congestion, frequent sinus infection-like episodes, facial pressure, or ongoing postnasal drip that never fully clears.
It’s also important to know that sinus symptoms can come from more than one cause. What feels like an infection might actually be inflammation, allergies, or even a structural blockage that prevents normal drainage. Research suggests nasal and sinus abnormalities can track with lupus disease activity—meaning more active lupus may be linked with more ENT-related findings in some patients.[1][2]
This guide is educational and designed to help you understand lupus and chronic sinus problems—what may drive them, how clinicians sort out the cause, and what treatment options are commonly considered. Medical note: This article is for general education and isn’t a substitute for personalized medical advice, diagnosis, or treatment. In short: sinus symptoms in lupus often stem from inflammation, infection risk, or anatomy—and good care starts with clarifying which of these is driving your symptoms.
Quick snapshot — Lupus and sinus issues at a glance
Common symptoms: nasal congestion or stuffiness; facial pressure (forehead/cheeks/between the eyes); postnasal drip and throat clearing; reduced sense of smell/taste; headache; fatigue and cough (often from drainage).
Most common drivers: autoimmune nasal inflammation (swelling without infection); higher infection risk from immune dysfunction and immunosuppressants; co-existing chronic rhinitis or chronic rhinosinusitis (CRS).
Why proper diagnosis matters: not every episode of sinus pressure and congestion is a bacterial infection. A “sinus infection” may actually be non-infectious inflammation that won’t improve with antibiotics—so getting the underlying cause right is key.[3][4] A simple way to think about it: antibiotics treat bacteria, but they don’t unblock the drain if swelling is the real issue.
How lupus (SLE) can affect the nose and sinuses
Autoimmune inflammation in the nasal lining
In lupus, the immune system can trigger inflammation in tissues throughout the body. In the nose and sinus region, that inflammation may irritate the nasal lining and narrow the tiny drainage pathways that keep sinuses ventilated. The result can be persistent swelling, blockage, and symptoms that mimic infection or allergies.[3][4]
An analogy many patients relate to: when drainage pathways get inflamed, they can behave like a pinched straw—air and mucus have trouble moving through, pressure builds, and you feel “stuck,” even if there’s no true infection.

Chronic rhinosinusitis (CRS) is more associated with SLE
Chronic rhinosinusitis (CRS) is typically defined as sinus-related symptoms lasting 12 weeks or longer, often with ongoing inflammation. Studies have found CRS is more strongly associated with SLE compared with the general population.[2] If you’re dealing with lupus and chronic sinus problems that seem to linger for months, learning about chronic rhinosinusitis can be a helpful starting point—especially if you’ve already tried multiple short-term fixes without lasting relief. Read more: https://sleepandsinuscenters.com/chronic-sinusitis
Lupus activity and nasal findings may be linked
One study found nasal symptoms and other nasal/sinus abnormalities in SLE patients were associated with higher disease activity markers (including higher SLEDAI scores and anti-dsDNA positivity).[1] While every person’s lupus is different, this supports an important concept: sinus and nasal symptoms may sometimes reflect what’s happening systemically. A practical takeaway: if your congestion and pressure flare around the same time as joint pain, fatigue, rash, or other lupus symptoms, that timing clue can help your clinicians connect the dots. Bottom line: when lupus flares, nasal and sinus inflammation can flare too—pay attention to patterns and share them with your care team.
Symptoms — What lupus-related chronic sinus problems can feel like

Nasal symptoms
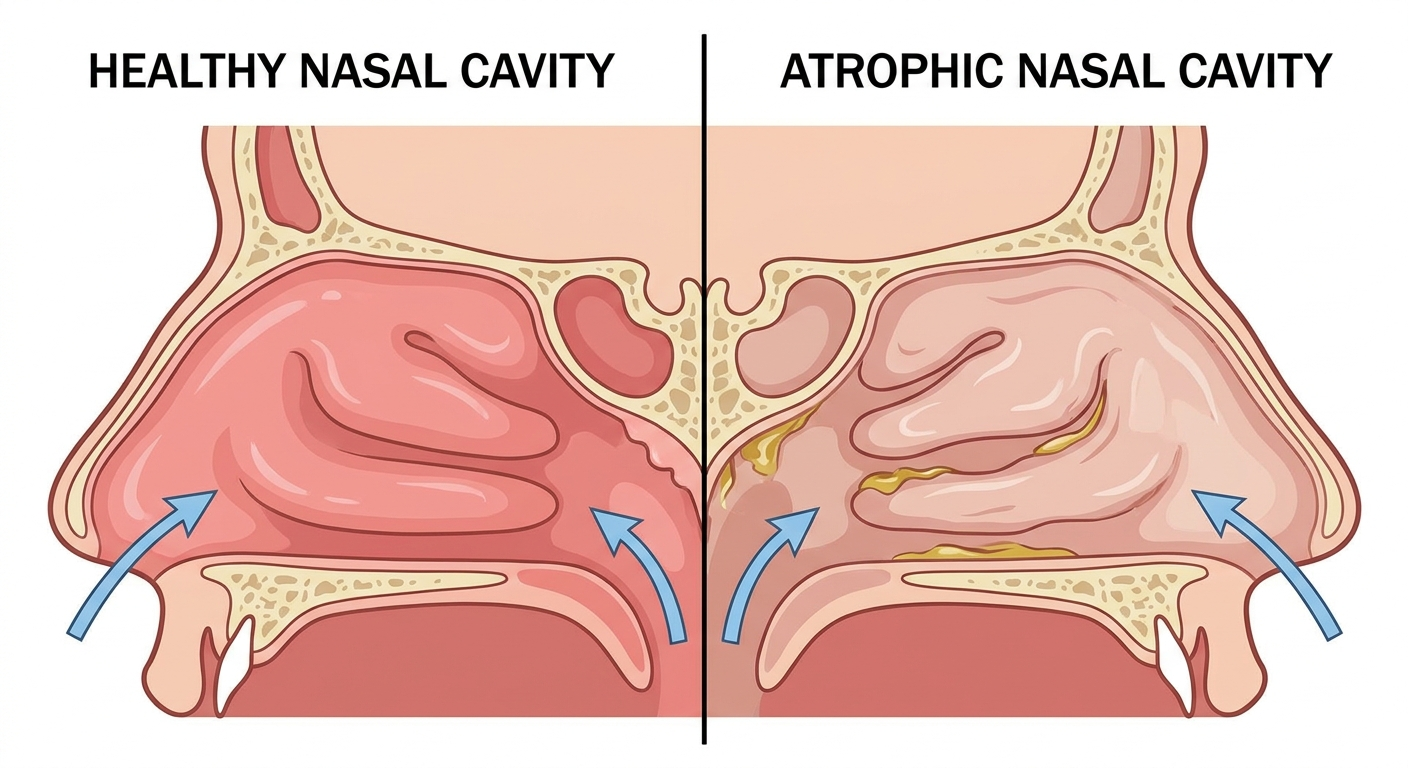
Nasal congestion (reported in 31.5% of SLE patients in one study)[1]; runny nose or thick drainage; sneezing and itching (more typical of an allergy pattern); dryness, crusting, or nosebleeds (sometimes influenced by medications, indoor air, or irritation). Some patients describe it like this: “My nose feels swollen shut even when I’m not sick, and the pressure comes and goes for weeks.” That pattern can fit chronic inflammation just as much as it fits repeated infections.
Sinus symptoms
Facial pressure or pain (cheeks, forehead, between the eyes); reduced smell/taste; ear pressure or fullness; bad breath.
Throat/chest/sleep-related symptoms (often overlooked)
Postnasal drip causing throat clearing or cough; mouth breathing, snoring, and poorer sleep due to blockage. When sleep quality drops, everything can feel harder—daytime fatigue, headaches, and brain fog may intensify. In lupus, where fatigue may already be a major symptom, addressing nighttime nasal obstruction can be especially meaningful.
Signs symptoms may be infection-related (not just inflammation)
Clinicians often become more concerned about bacterial infection when symptoms include fever; worsening one-sided facial pain/pressure; foul-smelling drainage; dental pain; or a pattern of temporarily improving, then rapidly worsening again. Because lupus and chronic sinus problems can involve both inflammation and infection, symptom patterns matter—and so does how quickly symptoms change. Key idea: long-lasting congestion often points to inflammation, while fast-escalating, focal pain with fever can suggest infection.
Causes — Why chronic sinus problems happen with lupus
1) Autoimmune-driven swelling (inflammation without infection)
Autoimmune inflammation may cause persistent swelling of the nasal lining and sinus outflow tracts. When swelling blocks drainage, mucus can accumulate—leading to pressure, congestion, and symptoms that can look like infection. In these cases, inflammation-focused strategies may be more effective than repeating antibiotics.[3][4] A common scenario: symptoms linger for weeks, and antibiotics bring little or only temporary improvement. That doesn’t prove there was no infection—but it does raise the possibility that inflammation and poor drainage play a major role.

2) Higher infection risk (immune system + medications)
Lupus can affect immune function, and many SLE treatment plans include therapies that suppress parts of the immune response. This combination can increase vulnerability to sinus infections, including infections that may feel more frequent or harder to clear. In this article, “lupus sinus infections” refers to sinus infections that occur more commonly or with greater severity due to lupus-associated immune changes, not a distinct infection type.[5] If you’re immunosuppressed, typical sinus symptoms should prompt earlier evaluation to rule out infection—especially if they escalate quickly or don’t follow your usual pattern.
3) CRS and chronic rhinitis overlap
CRS often overlaps with chronic rhinitis (persistent nasal inflammation). Symptoms can blur together—congestion, drainage, postnasal drip—but management isn’t always identical. If rhinitis is a major contributor, learn more here: https://sleepandsinuscenters.com/treating-chronic-rhinitis
4) Allergy triggers or irritants can add fuel
Seasonal pollen, dust, mold, smoke, and strong fragrances can worsen swelling and congestion—especially when the nasal lining is already sensitive. For people with recurrent or seasonal patterns, allergy testing may be part of clarifying what’s driving symptoms: https://sleepandsinuscenters.com/allergy-testing. In real life, many people have more than one trigger; for example, a baseline of autoimmune inflammation plus a spring pollen surge can create a “double hit.”
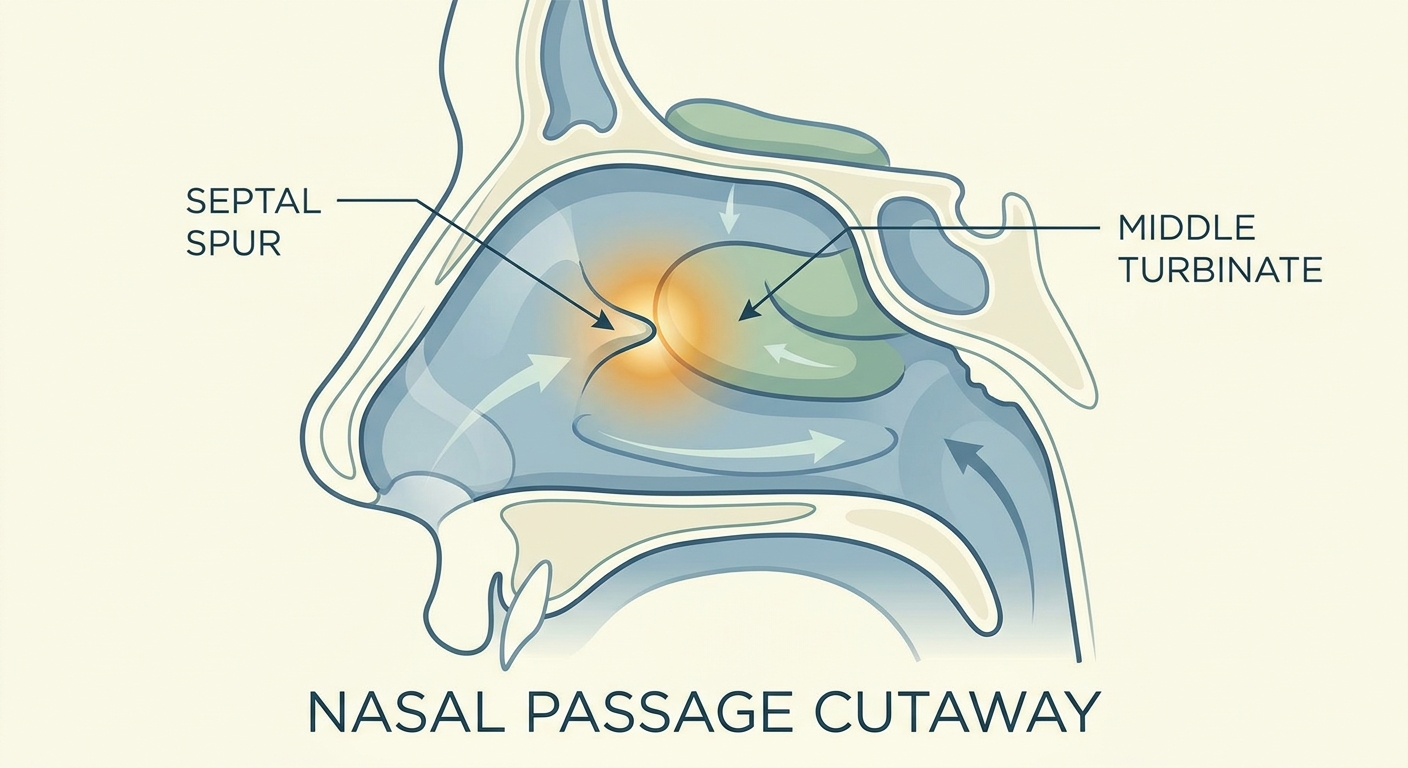
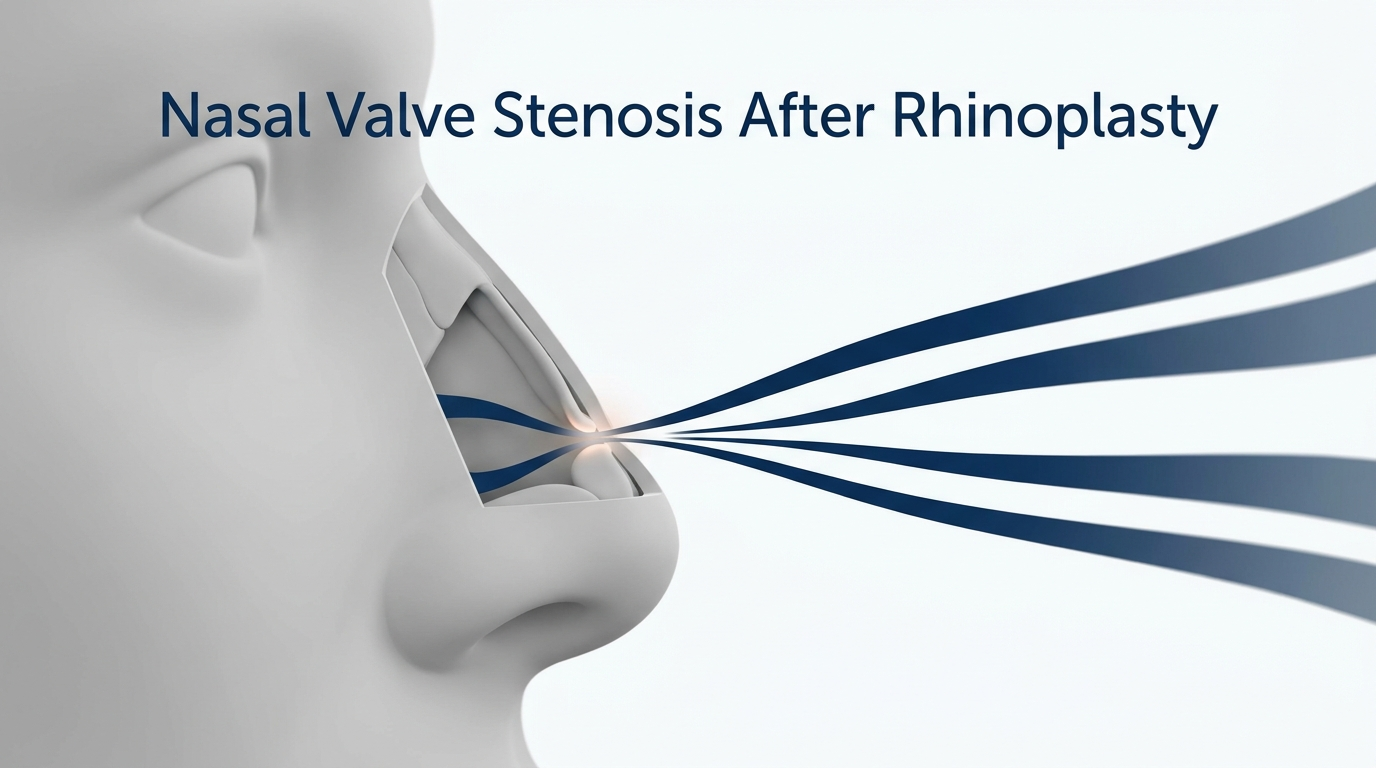
5) Structural/anatomical contributors
A deviated septum, enlarged turbinates, or nasal polyps (when present) can physically narrow airflow and drainage pathways. When structure and inflammation collide, symptoms can become persistent and more prone to flare. Takeaway: multiple factors—autoimmune inflammation, infection risk, allergies, and anatomy—often stack together to keep sinus symptoms going.
When to see a doctor urgently (red flags)
Seek urgent care for swelling/redness around the eye or vision changes; severe headache with neck stiffness; high fever, confusion, or severe facial swelling; rapidly escalating symptoms in someone who is immunosuppressed.
Diagnosis — How clinicians sort out lupus inflammation vs. infection
Medical history that matters
Key details include SLE history (recent flares, overall disease control); current medications (including steroids, DMARDs, biologics); how often infections occur and what treatments have or haven’t helped; allergy history and whether symptoms are seasonal or trigger-based. A short timeline of when symptoms started, what they felt like on day 1, and how they changed over time is very helpful.
Physical exam + ENT evaluation
An in-office nasal exam can look for swelling, crusting, polyps, and drainage patterns. When symptoms persist or the cause is unclear, clinicians may consider nasal endoscopy to get a closer view.
Imaging and tests (when needed)
Sinus CT may be used for chronic symptoms, to clarify the extent of inflammation, or for procedure planning. Allergy testing may be considered if symptoms fit an allergic pattern. Essentials: your story, an exam, and targeted testing help distinguish inflammation from infection and guide the right treatment.
Treatment options — What can help (and what to be careful about)
Because lupus treatment plans can be complex, it’s generally safest when ENT care and rheumatology care are coordinated—especially before any changes to immune-modulating medications.

Step 1 — Home and supportive care (often foundational)
Helpful basics include saline spray or irrigation (with proper technique and safe water); hydration and humidification (with good humidifier hygiene); trigger avoidance (smoke, strong fragrances, known allergens); rest and sleep positioning to reduce nighttime drainage. These simple measures often make other treatments work better—especially when dryness, crusting, or thick mucus is present.
Step 2 — Medications commonly used for chronic sinus inflammation
Depending on symptoms and drivers, options may include intranasal corticosteroid sprays to reduce swelling; if allergies play a role, antihistamines and/or nasal antihistamine sprays; short courses of oral steroids in select situations, weighing risks and benefits carefully in SLE and only under close medical supervision. Many patients notice that decreasing swelling improves breathing first—then pressure and drainage improve.
Step 3 — Treating sinus infections safely in lupus
Antibiotics may be appropriate when symptoms strongly suggest bacterial infection, but repeated courses aren’t always the best answer if the underlying problem is inflammatory CRS or ongoing autoimmune nasal inflammation.[3][4] Because medication interactions and immune status vary widely in SLE, treatment choices should be personalized—particularly when infections recur.
Step 4 — Coordinating care: controlling lupus to help the sinuses
For some patients, improved lupus control may reduce inflammation burden in the nose and sinuses. This is supported by research linking nasal/sinus findings with higher lupus activity markers.[1] Share timing patterns with both ENT and rheumatology teams.
Step 5 — Office procedures and surgical options (when meds fail)
If symptoms persist despite appropriate medical therapy—especially with frequent infections, ongoing blockage, or CT-confirmed disease—an ENT may discuss procedural options. Examples include balloon sinuplasty (a less invasive way to widen certain sinus drainage pathways in selected cases): https://sleepandsinuscenters.com/balloon-sinuplasty, and endoscopic sinus surgery for more extensive or complex disease.
Not everyone is a candidate; candidacy depends on anatomy, CT findings, and the specific type of sinus disease. For patients on immunosuppressive therapy, planning around procedures is individualized and typically involves careful perioperative coordination. Practical point: build from supportive care and medications, and consider procedures only when imaging, anatomy, and persistent symptoms clearly point that way.
Lifestyle tips to reduce flare-ups and infections

Build a “sinus-friendly routine”
Use saline regularly as recommended; use prescribed nasal sprays consistently; improve indoor air by reducing dust and mold, and avoid smoke and strong scents; keep humidifiers clean to prevent microbial buildup.
Infection prevention habits for immunosuppressed patients
Emphasize hand hygiene and practical exposure reduction during high-risk times; seek earlier evaluation when symptoms worsen, especially if you’re prone to complications or are on stronger immune-suppressing medications.[5]
Track patterns to spot triggers
Use a simple symptom diary to track weather/allergen exposure, lupus flare timing, medication changes, and sleep quality or snoring/mouth breathing. Brief notes—such as “pressure worse after rain,” “congestion flared with joint pain,” or “new med started last week”—can speed up diagnosis and reduce trial-and-error. Small daily habits and early check-ins during flares can meaningfully reduce symptom burden over time.
FAQs (patient-friendly, SEO-focused)
Can lupus cause chronic sinus inflammation even without an infection?
Yes. Lupus can contribute to persistent, non-infectious inflammation in the nasal passages and sinuses, and symptoms may not respond to infection-only treatment approaches.[3][4]
How can I tell if it’s allergies, a sinus infection, or lupus inflammation?
While overlap is common, patterns can help. Allergies: itching, sneezing, watery or clear drainage, seasonal triggers. Infection: fever, worsening one-sided pain, foul smell, thick discolored drainage, or initial improvement followed by rapid worsening. Lupus-related inflammation or CRS: persistent swelling or pressure, chronic congestion, limited response to repeated antibiotics.
Why do I get sinus infections more often on lupus medications?
Some lupus medications suppress the immune system to control inflammation. That suppression can also reduce infection-fighting capacity, which may increase susceptibility to sinus infections.[5]
Is chronic rhinosinusitis more common in SLE?
Research supports a higher association between SLE and CRS compared with the general population.[2] This connection is a key reason lupus and chronic sinus problems deserve a thoughtful, personalized evaluation.
When should I ask for an ENT referral?
Consider referral for symptoms lasting longer than 12 weeks; frequent or recurring infections; poor response to treatment; or when endoscopy or CT imaging is needed.
Can balloon sinuplasty help lupus patients with chronic sinusitis?
It may help when symptoms are driven by blockage and poor sinus drainage, but candidacy depends on anatomy, CT findings, and the type of sinus disease present. An ENT evaluation is needed to determine appropriateness.
Conclusion — Key takeaways and next steps
Lupus and chronic sinus problems often come down to a combination of ongoing inflammation and, for some patients, a higher risk of sinus infections, especially when immunosuppressive therapies are involved. Because symptoms can look similar whether the cause is infection, allergies, CRS, or autoimmune nasal inflammation, a clear diagnosis is the foundation of lasting relief.
If symptoms are persistent, severe, or recurrent, consider scheduling an evaluation so ENT and rheumatology care can be aligned—and so treatment can match the true driver of symptoms. To take the next step, you can book an appointment at Sleep & Sinus Centers of Georgia: https://www.sleepandsinuscenters.com. Next step: align ENT and rheumatology care, clarify the cause, and personalize treatment for durable relief.
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
1. Kusyairi et al. (2015). PubMed. https://pubmed.ncbi.nlm.nih.gov/26657735/
2. Rheumatology (Oxford Academic). https://academic.oup.com/rheumatology/article/63/1/149/7136653
3. Sleep & Sinus Centers of Georgia — Autoimmune disease & sinus inflammation. https://sleepandsinuscenters.com/blog/can-autoimmune-diseases-cause-sinus-inflammation-s-20260204121259
4. Top Doctors — Nasal inflammation/blockage in autoimmune diseases. https://www.topdoctors.co.uk/medical-articles/understanding-nasal-inflammation-and-blockage-in-autoimmune-diseases-causes-symptoms-and-treatment-options/
5. MyLupusTeam — Lupus and sinus infections. https://www.mylupusteam.com/resources/lupus-and-sinus-infections-is-there-a-connection
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.