Chronic Sinusitis Not Responding to Antibiotics: Causes, Treatments & Next Steps
If you’ve taken one (or several) rounds of antibiotics and still feel stuffed up, pressure-filled, and run down, you’re not alone. Chronic sinusitis not responding to antibiotics is common—and often confusing—because what feels like a lingering “infection” can actually be something different: long-term inflammation, blocked drainage, or even bacteria protected inside a sinus biofilm.
This article is educational (not personal medical advice). It’s meant to help you understand why symptoms persist and what evidence-based “next steps” typically look like—especially when you’re tired of repeating the same medication cycle.
Quick take: Why antibiotics often don’t “fix” chronic sinusitis
Antibiotics can be important in specific situations, but chronic rhinosinusitis (CRS) is frequently driven more by inflammation than an ongoing, straightforward bacterial infection—so antibiotics may only help briefly or not at all. [1][2]
A few key reasons:
- Inflammation is often the main problem. In CRS, the sinus lining can stay swollen and reactive for months, which keeps symptoms going even when bacteria aren’t the primary driver. [1][2]
- Biofilms can contribute to “treatment failure.” In CRS, bacteria may live in biofilms—protective communities that are harder for antibiotics to penetrate and harder for the immune system to clear. [3][4]
- Repeated antibiotics have downsides. Multiple courses can raise the risk of side effects and contribute to antibiotic resistance, without addressing the underlying inflammation or blockage. [1][2]
Think of it this way: antibiotics can help when the problem is “germs in the mucus,” but they can’t fully solve “swollen lining + poor drainage.” If the sinus openings are narrowed, it’s like trying to mop up an overflowing sink without unclogging the drain.
Mini-preview: If your symptoms keep coming back, the next step is usually a more precise diagnosis (endoscopy/CT/allergy evaluation) and anti-inflammatory and mechanical therapies (e.g., saline irrigation and steroid nasal spray), sometimes combined with procedures to improve drainage.
Bottom line: If antibiotics keep falling short, shift the focus to inflammation control and better sinus drainage.

What counts as “chronic” sinusitis (and how it differs from acute infections)
CRS definition (patient-friendly)
CRS generally means sinus symptoms lasting 12 weeks or longer, plus objective evidence of inflammation seen on nasal endoscopy and/or a CT scan. [1]
If you want a deeper overview, Sleep and Sinus Centers of Georgia also has a helpful hub on chronic sinusitis symptoms and causes: https://sleepandsinuscenters.com/chronic-sinusitis
Why acute sinus infections and CRS behave differently
Acute sinusitis is often related to viral illness, and only a subset becomes bacterial. [2] CRS, on the other hand, is usually a long-term inflammatory condition with flare-ups—more similar to an ongoing airway problem than a one-time infection. [1][2]
A practical example: an acute infection might hit hard for a week and then clear. CRS often lingers as “always congested, always dripping, always pressure,” with occasional worse days that feel like a new infection.
You can also explore acute vs chronic sinusitis differences here: https://sleepandsinuscenters.com/blog/acute-vs-chronic-sinusitis-key-differences-and-treatment-options
If symptoms persist beyond 12 weeks, think CRS—not just a lingering cold or one-off infection.
Symptoms: Signs your “sinus infection” may actually be chronic inflammation
Common CRS symptoms (with/without nasal polyps) [1]
- Nasal congestion/obstruction
- Thick drainage (from the front of the nose and/or postnasal drip)
- Facial pressure or fullness (not always true “pain”)
- Reduced smell or taste
- Cough, throat clearing, fatigue, and poor sleep (often secondary effects)
Many people describe a “heavy face” sensation, constant throat clearing, or waking up tired because they can’t breathe well at night.
Clues antibiotics won’t help much
When symptoms of sinus infection do not respond to antibiotics, these patterns often occur:
- Symptoms improve briefly, then return soon after finishing antibiotics
- Congestion and pressure dominate, with little or no fever
- A long history of allergies or asthma
- Persistent smell loss (especially when nasal polyps are involved) [1][2]
A clinician-style way of saying it: “If each antibiotic works…until it doesn’t, it’s time to treat what’s underneath the flares.”
Red flags—seek urgent care
Some symptoms require prompt evaluation, because complications (while uncommon) can be serious: [2]
- Swelling around the eye, vision changes
- Severe headache, stiff neck
- High fever with worsening symptoms
- Confusion, severe facial swelling
- Higher-risk situations such as immune compromise
If antibiotics only nudge your symptoms temporarily, inflammation and drainage issues may be the real culprits.

Why chronic sinusitis may not respond to antibiotics (top causes)
When people search chronic sinusitis not responding to antibiotics, they’re often dealing with one (or more) of these underlying issues:
1) CRS is inflammatory—not primarily infectious
In many cases, the biggest driver is swollen, inflamed sinus lining and ongoing immune signaling—not “free-floating” bacteria that antibiotics can easily eliminate. [1][2]
2) Biofilms and “protected bacteria”
A sinus biofilm is a structured community of bacteria protected by a matrix that can resist antibiotics and immune clearance. [3][4] Biofilms may help explain why some people feel partially better during treatment and then relapse.
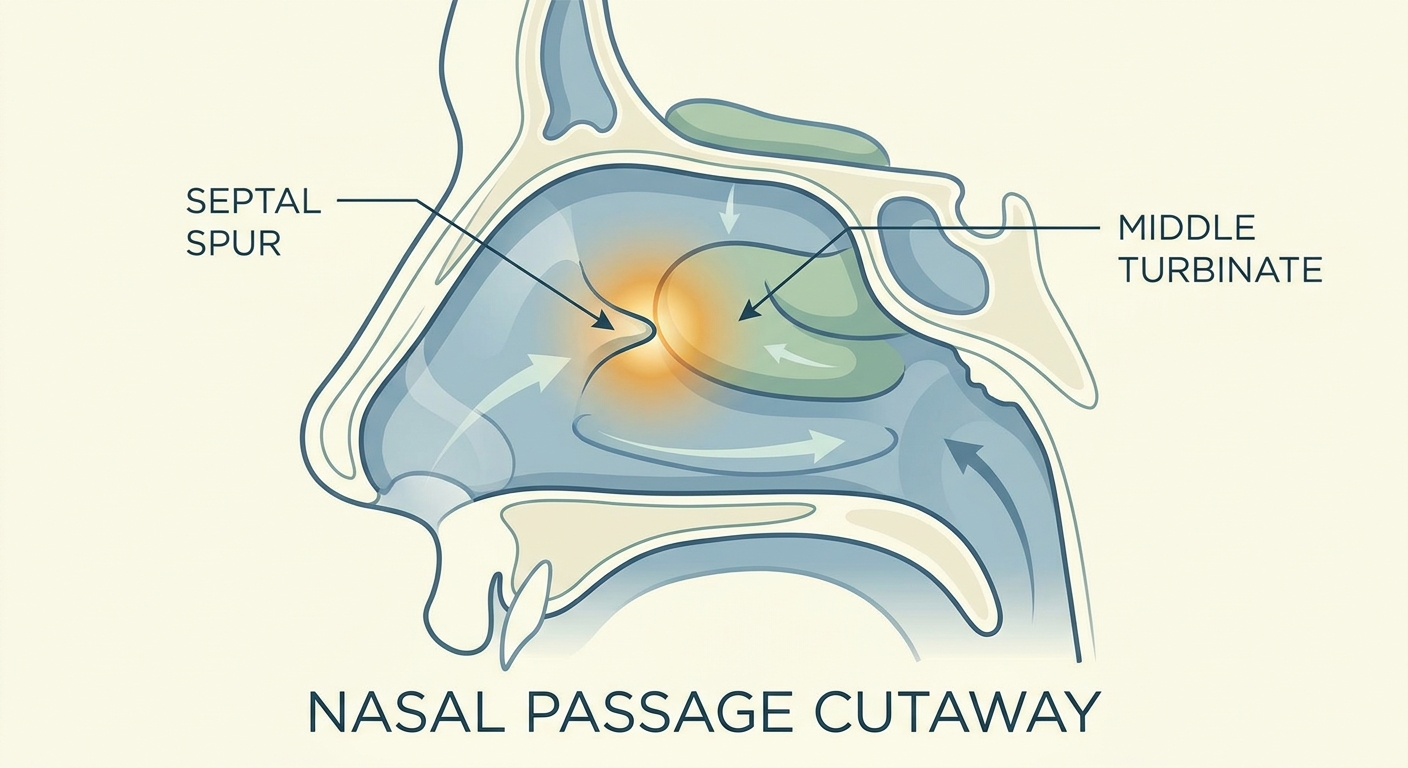
3) Structural blockage that prevents drainage
Even the best medication has trouble working if mucus can’t drain well. Common contributors include: [1]
- Deviated septum
- Turbinate enlargement
- Narrow natural drainage pathways
- Nasal polyps or swelling that closes sinus openings
4) Allergies and ongoing trigger exposure
Allergens like dust mites, pollen, mold, and pet dander can keep the nose inflamed and reactive, setting the stage for persistent symptoms. [1]
5) Non-bacterial mimics (often missed)
Some “sinus” complaints aren’t actually bacterial sinusitis. Examples include: [1]
- Nonallergic rhinitis
- Migraine (often mistaken for “sinus headache”)
- Dental sources (upper molar problems can refer pain/pressure)
- Selected fungal-related conditions, including allergic fungal sinusitis
6) Antibiotic resistance or wrong target organism (less common than people think)
True persistent bacterial infection can happen, but repeated empiric antibiotics without a targeted approach can miss the organism (or the real cause). [2][3]
CRS often persists because of inflammation, anatomy, and biofilms—factors antibiotics alone can’t fix.

Next steps: How an ENT figures out what’s really going on
History + symptom pattern
Clinicians often look at:
- How long symptoms have lasted
- Seasonal or trigger patterns
- Prior medication trials and response
- Coexisting asthma/eczema, reflux symptoms, or irritant exposure
Nasal endoscopy (in-office)
Endoscopy can identify polyps, drainage, swelling, and anatomy issues, and may help guide cultures in selected situations. [1]
CT scan of the sinuses
A CT scan can show chronic inflammation patterns and structural blockages. It’s also commonly used when planning procedural options. [1]
Allergy evaluation (when appropriate)
Testing may be useful when symptoms are persistent, seasonal, or clearly trigger-linked. [1]
When a culture is helpful
Cultures may be considered with recurrent or severe flare-ups, immune compromise, or failure of standard therapy—especially when a more targeted plan is needed. [1][2]
An ENT workup (history, endoscopy, CT, and sometimes allergy testing) clarifies the root causes so treatment can match the problem.

Treatments that work when antibiotics don’t (evidence-based options)
Goal: reduce inflammation, improve drainage, and restore healthier nasal function.
Foundation therapy #1 — Nasal saline irrigation (daily)
Saline irrigation helps wash out mucus, allergens, and inflammatory debris, and is a cornerstone of CRS care. [1]
Practical pointers often emphasized include:
- Use distilled, sterile, or previously boiled and cooled water
- Keep the device clean and allow it to dry
- Consistent technique matters more than occasional “rescue” rinses
Many patients do best by pairing the rinse with an existing habit (after brushing teeth, post-shower, or before bed) so it becomes routine rather than something you only try when you’re miserable.
For a practical guide, see how often should you use nasal rinses: https://sleepandsinuscenters.com/blog/nasal-rinses-how-often-should-you-use-them
Foundation therapy #2 — Intranasal corticosteroid sprays
A steroid nasal spray can reduce inflammation and help control polyp growth for many people with CRS. It’s often used as maintenance therapy. [1][2]
Technique can make a big difference. Common tips include:
- Aim slightly outward (toward the ear), not straight up or toward the septum
- Use gentle sniffing (avoid “snorting” it down the throat)
Step-by-step help: steroid nasal spray technique: https://sleepandsinuscenters.com/blog/steroid-nasal-spray-technique-step-by-step-guide-for-effective-use
Steroid irrigations (for selected patients)
Under clinician guidance, steroid can sometimes be delivered via irrigation for broader distribution than sprays in certain scenarios (often after surgery). [1]
Short oral steroids (carefully selected cases)
In some cases—especially significant inflammation or polyps—short courses may be considered. Because risks and benefits vary, this is usually a clinician-guided decision. Common side effects can include mood or sleep changes, elevated blood sugar or blood pressure, fluid retention, and reflux flares.
Address contributors: allergies, asthma, reflux, irritant exposure
CRS management often works best when contributing issues are addressed, such as:
- Allergen avoidance strategies and appropriate allergy medications (when allergic)
- Asthma optimization (upper and lower airway often influence each other)
- Reducing irritant exposure (smoke, strong fragrance)
What the evidence says about antibiotics in CRS
Antibiotics are not considered a cure for CRS. They may be reserved for acute bacterial exacerbations or specific scenarios, rather than repeated empiric courses without reassessment. [1][2]
This is why chronic sinusitis not responding to antibiotics is often a sign to “zoom out” and treat CRS as a long-term inflammatory condition.
Consistent saline rinses plus intranasal steroids are the backbone; reserve antibiotics for true bacterial flares.
Non-antibiotic antimicrobials & emerging options (what’s promising, what’s experimental)
Xylitol nasal irrigation (adjunct option)
A xylitol nasal rinse is sometimes discussed as an adjunct. Some research suggests xylitol may reduce bacterial adhesion/biofilm behavior and improve symptoms for certain patients, though it’s not a universal solution. It’s worth discussing with an ENT—especially if you have sensitive nasal tissue. [5][6]
Bacteriophages (research stage)
Phage therapy is being investigated for biofilm-related and resistant infections. It’s not standard CRS care yet, but it’s an area researchers are actively exploring. [7]
Why “natural antibiotics” aren’t always the answer
Many over-the-counter “antimicrobial” supplements lack strong CRS-specific evidence. These supplements should not replace established therapies. [2]
Adjuncts can help some patients, but core anti-inflammatory care remains the most reliable strategy.

When procedures help: Balloon sinuplasty vs endoscopic sinus surgery (ESS)
Signs you might benefit from a procedure
A procedure may be considered when:
- Symptoms persist despite guideline-based medical therapy
- CT shows blocked drainage pathways
- Flares frequently disrupt sleep, work, or quality of life [1]
Balloon sinuplasty (less invasive option for selected anatomy)
Balloon sinuplasty uses a balloon to widen the natural sinus openings to support better drainage. It’s often considered in selected cases of chronic blockage without extensive polyps. [8]
Learn more at Sleep and Sinus Centers of Georgia: balloon sinuplasty for chronic sinus blockage: https://sleepandsinuscenters.com/balloon-sinuplasty
Endoscopic sinus surgery (ESS)
Endoscopic sinus surgery can remove obstruction and improve ventilation/drainage. A major benefit is often improved ability for topical medications (like irrigations and sprays) to reach target areas afterward. [1]
Related read: endoscopic sinus surgery (ESS) for chronic sinusitis: https://sleepandsinuscenters.com/blog/endoscopic-sinus-surgery-what-patients-should-know
What “success” looks like
In CRS, “success” often means:
- Fewer flare-ups
- Improved breathing and/or smell
- Better sleep
- Less need for antibiotics—paired with ongoing maintenance care [1]
If medicines aren’t enough, procedures that open drainage pathways can make your daily treatments work better.
Lifestyle & home-care tips to reduce flare-ups (practical and patient-friendly)
Daily habits that support sinus health
- Keep a consistent routine with irrigation and nasal spray (as directed)
- Stay hydrated
- Consider humidification when indoor air is dry
- Pay attention to sleep positioning if postnasal drip is a frequent issue
Reduce exposure to triggers
- Dust-mite control (bedding covers, hot-water washes)
- HEPA filtration
- Mold mitigation
- Avoid smoke and strong fragrances
- During high-pollen days: shower, change clothes, and consider rinsing
Medication safety reminders
- Avoid long-term use of topical decongestant sprays (rebound congestion can occur)
- Use antibiotics only when clearly indicated to help reduce resistance risk [2]
Small, consistent habits—plus trigger reduction—can curb flares and improve day-to-day breathing.
FAQs
Why do antibiotics help my sinus symptoms for a few days, then they come back?
Temporary improvement can happen, but CRS often persists because the underlying issue may be inflammation, drainage problems, and/or biofilms—not an easily eradicated infection. [1][3]
Does green mucus mean I need antibiotics?
Not necessarily. Mucus color alone doesn’t reliably distinguish viral vs bacterial vs inflammatory causes. [2]
How long is too long to have sinus symptoms?
If symptoms last 12 weeks or more, or you keep relapsing, it’s reasonable to ask about CRS evaluation (endoscopy/CT). [1]
What is a sinus biofilm?
A sinus biofilm is a structured community of bacteria protected by a matrix that can resist antibiotics and immune clearance. [3][4]
What’s the best treatment for chronic sinusitis?
Often it’s a combination of saline irrigation + intranasal steroids, trigger management, and sometimes a procedure when obstruction persists. [1][2]
When should I see an ENT?
Consider evaluation when symptoms persist beyond 12 weeks, recur frequently, smell is reduced, polyps are suspected, or when chronic sinusitis is not responding to antibiotics and quality of life is affected. [1][2]
In CRS, the most effective plan treats inflammation first, improves drainage, and personalizes care based on your anatomy and triggers.
Conclusion: Your action plan if chronic sinusitis isn’t improving
If you’re dealing with chronic sinusitis not responding to antibiotics, an effective next step is usually a clearer diagnosis and a CRS-focused plan:
1) Confirm whether it’s CRS vs recurrent acute infections
2) Commit to daily anti-inflammatory + rinse therapy (not just antibiotics)
3) Consider an ENT workup (endoscopy/CT/allergy) to identify biofilms, polyps, or blockage
4) If structural issues persist, discuss procedural options like balloon sinuplasty or endoscopic sinus surgery [1]
If you’re ready for a specialist evaluation, you can book an appointment with Sleep and Sinus Centers of Georgia here: https://www.sleepandsinuscenters.com/
If you’re looking for more on what happens when standard care hasn’t worked, see: what to do after chronic sinusitis medical treatment fails: https://sleepandsinuscenters.com/blog/failed-chronic-sinusitis-medical-management-next-t-20260128051047
A targeted diagnosis plus consistent, inflammation-focused care is the best path out of the antibiotic cycle.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
1. AAFP (2017) — Chronic Rhinosinusitis overview/guidance. https://www.aafp.org/pubs/afp/issues/2017/1015/p500.html
2. Cochrane Review — Interventions in chronic rhinosinusitis (evidence summaries). https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD011994.pub2/full
3. PubMed (2016) — Biofilms and CRS (overview and clinical implications). https://pubmed.ncbi.nlm.nih.gov/27863163/
4. PMC — Biofilms in CRS and resistance background. https://pmc.ncbi.nlm.nih.gov/articles/PMC3836217/
5. SAGE Journals — Xylitol/topical approaches discussion. https://journals.sagepub.com/doi/10.1177/0145561319849421
6. ScienceDirect (2024) — Non-antibiotic antimicrobial strategies and CRS research. https://www.sciencedirect.com/science/article/pii/S180886942400051X
7. Frontiers in Microbiology (2020) — Bacteriophages, biofilms, antimicrobial alternatives. https://www.frontiersin.org/journals/microbiology/articles/10.3389/fmicb.2020.595555/full
8. Patient-facing overview of procedural options when antibiotics don’t work. https://www.americansinus.com/blog/sinusitis-what-to-do-if-antibiotics-dont-work-2
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.