Sleep Study for Insomnia: Diagnosis, What to Expect, and Treatment Options
Insomnia is common and often treatable. If you’re staring at the ceiling at 2 a.m. or waking up too early and feeling drained all day, it’s natural to wonder whether you need a sleep study for insomnia.
Here’s the key: most insomnia is diagnosed clinically (through your history and sleep patterns), and a sleep study is not routinely required. But in certain situations, testing can be very helpful—especially when symptoms suggest another sleep disorder (for example, to distinguish sleep apnea from insomnia) or when insomnia doesn’t improve with first-line treatment.
Note: In most cases, a careful history plus proven treatment is enough; testing is reserved for specific situations.
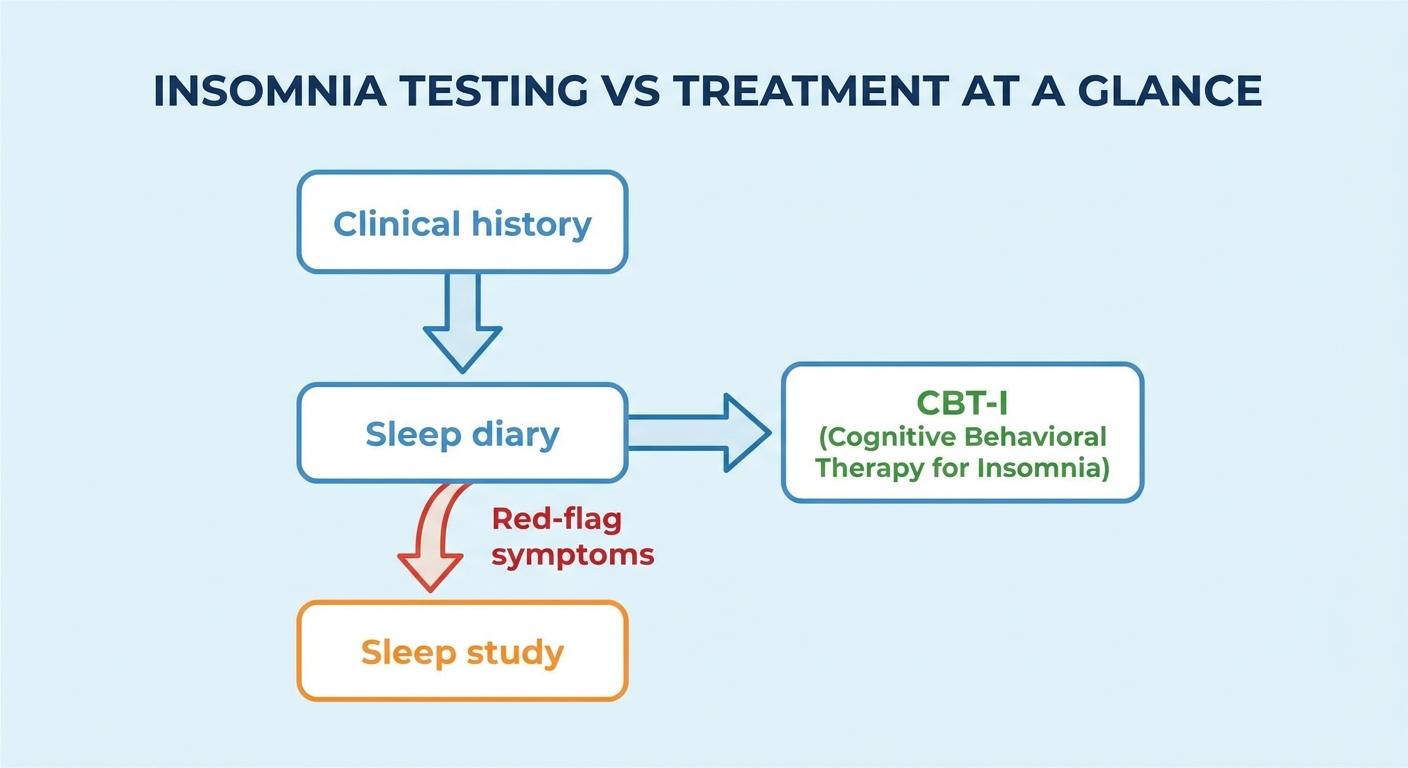
Insomnia Testing vs Treatment: At a Glance
- Most common path: clinical insomnia diagnosis + sleep diary → CBT‑I for chronic insomnia
- A sleep study is most useful when another sleep disorder may be contributing to the symptoms
- Home sleep tests primarily evaluate sleep apnea, not insomnia itself
- Wearables are helpful for trends, but accuracy is limited for quiet wakefulness
- Best‑supported first‑line treatment for chronic insomnia: CBT‑I
Do You Need a Sleep Study for Insomnia?
Many people assume a sleep study is the “standard test” for insomnia. In reality, the best next step depends on why you’re not sleeping and what your symptoms look like.
A sleep study may be recommended to rule out other sleep disorders or to clarify stubborn, complex sleep complaints. Think of it like this: insomnia is often diagnosed the way clinicians diagnose migraines or reflux—by the pattern of symptoms over time—while sleep studies are most useful when we need to measure breathing, movements, or unusual nighttime events. Testing decisions ultimately depend on a clinician’s assessment of your full history and risk factors.
This article walks through:
- what insomnia is and why it happens,
- when testing helps,
- what a sleep study is like,
- how results are interpreted, and
- what treatments actually work.
Note: Start with your story and symptoms; add testing only when it’s likely to change the plan.
What Is Insomnia (and When Is It “Chronic”)?
Quick definition (simple, patient‑friendly)
Insomnia means difficulty:
- falling asleep, staying asleep, waking too early, and/or
- getting non‑restorative sleep,
plus daytime impact (fatigue, mood changes, concentration issues, etc.).
Clinicians often describe insomnia as:
- short‑term (acute): days to weeks
- chronic: symptoms at least 3 months, typically occurring multiple nights per week
Why insomnia isn’t just “not enough sleep”
Insomnia isn’t always about “needing more sleep time.” It often reflects an imbalance between:
- sleep drive (your body’s pressure to sleep), and
- the brain’s alerting system (wake/attention signals)
A common pathway is hyperarousal insomnia—your mind and body behave as if they need to stay on guard. That can look like racing thoughts, a “tired but wired” feeling, or a sudden spike of alertness when you lie down. A clinician might say: “Your sleep system is ready, but your threat‑detection system is still on.” That framing matters, because it points to treatments that retrain the system—rather than just “trying harder” to sleep.
Note: Insomnia is a pattern of nighttime difficulty plus daytime impact, often driven by a brain that’s too alert at bedtime.
Common Symptoms of Insomnia (Day and Night)
Nighttime symptoms
- Taking a long time to fall asleep
- Frequent awakenings
- Waking earlier than intended
- Worry, frustration, or dread about sleep
Daytime symptoms
- Fatigue, low energy
- Mood changes, irritability
- Concentration or memory issues
- Reduced performance at work or school
- Increased reliance on caffeine
When symptoms suggest evaluation beyond insomnia
Some symptoms raise the likelihood of a different (or additional) sleep disorder:
- Loud snoring, witnessed pauses in breathing, choking/gasping (possible sleep apnea)
- Uncomfortable leg sensations or urge to move (possible RLS/PLMD)
- Dream enactment, sleepwalking, unusual nighttime behaviors (parasomnias)
- Persistent reflux, nasal obstruction, or chronic cough disrupting sleep
When these show up, a sleep study may be ordered—not because insomnia “needs” a sleep study, but because another condition may be driving the awakenings. Many patients say some version of: “I thought I just couldn’t sleep…until someone noticed my breathing.” That’s exactly the scenario where testing can change the plan in a meaningful way.
Note: Clues like snoring, gasping, limb movements, or unusual behaviors often point to testing for other sleep disorders.
What Causes Insomnia? (The Most Common Drivers)
Behavioral + schedule factors
- Irregular sleep and wake times
- Napping (especially late‑day)
- Spending extra time in bed trying to “catch up”
One common example: going to bed earlier to “get ahead” after a bad night. It’s understandable—but spending long stretches awake in bed can weaken the bed‑sleep connection and worsen insomnia over time.
Stress, anxiety, and learned insomnia patterns
Over time, insomnia can become learned and self‑reinforcing:
- The bed becomes associated with wakefulness (conditioned arousal)
- Rumination and performance pressure (“I have to sleep or tomorrow is ruined”)
This is why insomnia often feels bigger than the original trigger. Even after stress improves, the brain can keep “checking” for sleep—ironically making sleep harder to access.
Medical and sleep‑related contributors
- Obstructive sleep apnea (OSA)
- Chronic pain, menopause symptoms, thyroid issues
- Anxiety/depression (bidirectional relationship)
- Medications/substances (stimulants, nicotine, alcohol)
Environmental contributors
- Noise, light, temperature
- Partner sleep disruptions
- Travel, shift work, or circadian misalignment
Note: Insomnia usually reflects a mix of habits, stress patterns, and medical factors that keep the brain too alert at night.
Is a Sleep Study Required to Diagnose Insomnia?
Usually, no. Insomnia is typically diagnosed through:
- a detailed sleep history interview,
- a sleep diary (often 1–2 weeks), and sometimes
- questionnaires such as the Insomnia Severity Index (ISI).
A common misconception is: “If my sleep study looks normal, my insomnia isn’t real.” That’s not true. Polysomnography is not required for routine insomnia diagnosis, and its main role is to evaluate for other sleep disorders or select complex cases. A recent review discusses this evolving role in more detail: Polysomnography in Transition (2025). https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
Also important: a sleep study is a snapshot. Your lived experience—patterns across many nights plus daytime impact—is often the most clinically meaningful “data set.”
Note: Insomnia is usually diagnosed from your history and sleep diary, with testing added only when it’s likely to change care.
When a Sleep Study Is Helpful for Insomnia
You might need testing if another sleep disorder is suspected
A clinician may recommend polysomnography when they suspect:
- Sleep apnea (snoring, witnessed apneas, gasping)
- Significant, unexplained daytime sleepiness (more than just “tired”)
- Kicking/jerking movements during sleep or restless legs symptoms
- Parasomnias such as dream enactment or sleepwalking
Insomnia that doesn’t improve with first‑line treatment
If you’ve had an adequate trial of CBT‑I (including high‑quality digital CBT‑I) and sleep is still severely disrupted, testing can help identify “hidden” contributors—especially breathing or movement‑related arousals that are easy to miss from symptoms alone.
Complex or higher‑risk situations
Some medical conditions and safety‑critical jobs may prompt a more comprehensive evaluation. Testing decisions are individualized and based on the full clinical picture.
Research/advanced phenotyping (brief)
Specialized settings may use advanced EEG features (like ORP and hypnodensity) or multi‑night recordings to better characterize insomnia subtypes and monitor treatment response. Review (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
Note: Testing helps most when red‑flag symptoms or persistent problems suggest another sleep disorder may be involved.
Types of Sleep Studies and Monitoring Tools (What Your Doctor Might Order)
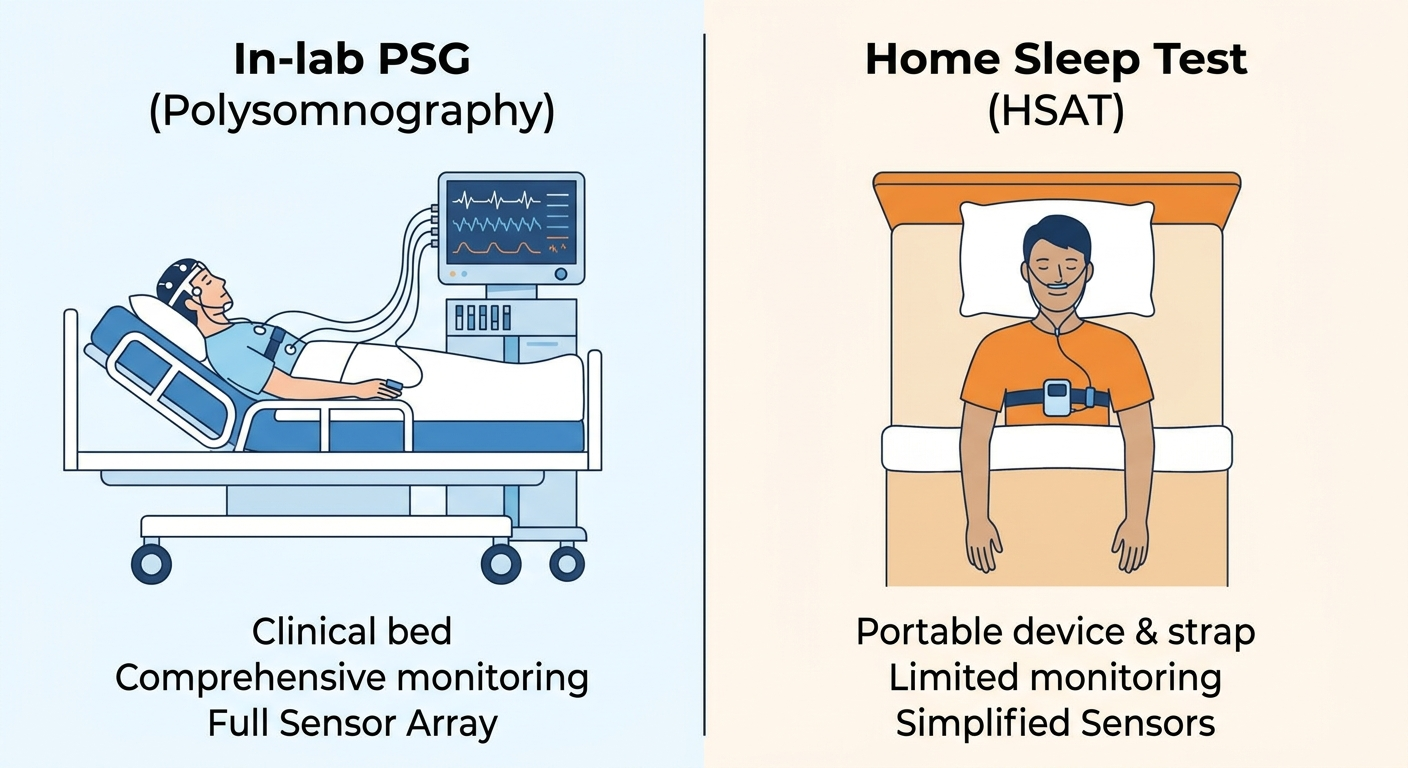
In‑lab polysomnography (PSG)
An in‑lab PSG records brain waves (EEG), breathing, oxygen levels, heart rhythm, and limb movements. It’s typically best for complex cases—especially parasomnias, movement disorders, or suspected apnea with additional medical concerns.
For a deeper comparison, see: Home sleep test vs. lab study. https://sleepandsinuscenters.com/blog/home-sleep-test-vs-lab-study-which-sleep-test-is-best-for-you
Home sleep apnea test (HSAT)
An HSAT is designed primarily to detect sleep apnea, not insomnia itself. It usually does not capture the same brain‑wave detail as an in‑lab PSG, so it may miss subtle sleep‑wake patterns.
For expectations and limitations: How accurate are home sleep tests? https://sleepandsinuscenters.com/blog/home-sleep-test-accuracy-how-reliable-are-at-home-sleep-tests
Actigraphy (watch‑like medical device)
Actigraphy estimates sleep/wake based on movement over many nights. It can be useful for circadian rhythm concerns and documenting night‑to‑night variability—especially when the goal is to understand patterns (like weekday vs weekend sleep) rather than label a single night as “good” or “bad.”
Consumer wearables (smartwatches/rings) — helpful but not definitive
Wearables can be great for spotting trends (bedtime consistency, sleep duration patterns). But accuracy can be limited, especially because quiet wakefulness is often mislabeled as sleep. They’re improving, but they’re not a full replacement for targeted testing in complex cases. Review (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
Related read: Limitations of watch‑style sleep tests https://sleepandsinuscenters.com/blog/watch-style-sleep-tests-key-limitations-you-need-to-know
Note: Choose the test that answers the specific clinical question—often apnea screening first, lab testing for complex cases.

What to Expect During a Sleep Study (Step‑by‑Step)
Before your study
Common instructions may include:
- Avoiding naps (if asked)
- Limiting caffeine later in the day (if instructed)
- Keeping a typical schedule leading up to the study
If you take medications, ask the sleep team what to do—stopping certain meds abruptly may not be appropriate. Bring comfortable sleep clothes, toiletries, and something relaxing (book, charger).
Arrival and setup
Sensors are placed on the scalp and body to monitor sleep and breathing. It’s noninvasive, and you’ll have privacy in a bedroom‑like setting. Many labs aim for “comfortable, not clinical.” If you’re worried about the wires, it may help to remember the goal is measurement, not perfection—you don’t need to sleep well for the study to be useful.
Overnight experience
Many people worry they “won’t sleep at all.” That’s common. Even imperfect sleep can still provide useful information about breathing events, oxygen levels, movements, and arousals. If anxiety spikes, tell the technologist.
After the study
In the morning, sensors are removed and you head home. Results are typically reviewed and interpreted after scoring—often within 1–2 weeks, depending on scheduling.
Note: Even if you sleep less than usual, a study can still capture valuable data about breathing, movements, and arousals.
Understanding Sleep Study Results (Without the Jargon)
Key PSG terms you may see
- Sleep latency: time it takes to fall asleep
- WASO: wake after sleep onset
- Sleep efficiency: percent of time in bed spent asleep
- Sleep stages: N1/N2/N3/REM
- AHI/RDI: breathing‑event indices used for sleep apnea severity
If your report includes AHI, this explainer can help: AHI score explained https://sleepandsinuscenters.com/blog/ahi-score-explained-understanding-your-sleep-apnea-severity
Why results can look “normal” in insomnia
- Quiet wakefulness can be hard to interpret without your diary and symptoms
- A one‑night lab study may not reflect typical home sleep (“first‑night effect”)
- Insomnia is often defined by the combination of sleep difficulty and daytime impact—not just the numbers
Emerging/advanced metrics (brief)
Measures like qEEG spectral analysis, spindles, ORP, and hypnodensity are promising for subtyping insomnia and tracking change, but they’re still evolving and require more validation. Review (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
Note: Numbers help, but your multi‑night pattern and daytime impact matter most for diagnosing insomnia.
Treatment Options After Diagnosis (What Actually Works)
First‑line treatment: Cognitive Behavioral Therapy for Insomnia (CBT‑I)
For chronic insomnia, CBT‑I is the recommended first‑line approach. It targets the thoughts and behaviors that keep insomnia going, such as conditioned arousal and unhelpful sleep routines.
CBT‑I commonly includes:
- Sleep scheduling (often called sleep restriction therapy)
- Stimulus control (retraining the bed/brain association)
- Cognitive strategies (reducing catastrophic sleep thoughts)
- Relaxation skills
- Sleep hygiene as support (helpful, but rarely sufficient alone)
According to recent AASM guidance, CBT‑I is the foundation of care for chronic insomnia. https://aasm.org/combination-treatment-chronic-insomnia-guideline
Digital/eHealth CBT‑I (app or online programs)
Digital CBT‑I can broaden access—especially for busy schedules or limited local availability. Studies show digital/eHealth CBT‑I has shown clinically meaningful benefit and may be comparable to in‑person CBT‑I for many outcomes, depending on the program and patient population. (JMIR 2024) https://mental.jmir.org/2024/1/e58217/ Meta‑analyses also show consistent benefit, though dropout varies by program design and support level. https://pmc.ncbi.nlm.nih.gov/articles/PMC12965280/
What to look for:
- a structured CBT‑I program (not just general sleep tips),
- clear week‑by‑week guidance,
- reminders or optional coaching if you tend to lose momentum.
Medications for insomnia (when they’re used)
Medication may be used as a short‑term, targeted tool in selected situations—particularly when symptoms are severe or while CBT‑I skills are being established. Risks can include next‑day impairment, falls risk (especially in older adults), and interactions with alcohol or other sedatives. Talk with a clinician to weigh pros and cons for your situation.
CBT‑I plus medication (combination therapy): when it makes sense
Recent AASM guidance suggests CBT‑I plus medication may offer modest benefits over medication alone, but does not recommend routine combination therapy compared with CBT‑I alone. https://aasm.org/combination-treatment-chronic-insomnia-guideline
Treat comorbid sleep disorders (often the missing piece)
If testing reveals a contributor such as sleep apnea or limb‑movement‑related sleep disruption, treating that condition can reduce awakenings and improve sleep quality. This is one of the main reasons a sleep study can be valuable in the right scenario.
Note: Build your plan on CBT‑I, add medication selectively if needed, and treat any comorbid sleep disorders uncovered by testing.

Lifestyle Tips That Support Treatment (Without Overselling “Sleep Hygiene”)
Helpful habits (supportive, not curative alone)
- Keep a consistent wake time (your “anchor”)
- Get morning light exposure
- Set a caffeine cut‑off that doesn’t spill into late afternoon/evening
- Limit alcohol near bedtime (it can worsen awakenings)
- Make the bedroom dark, cool, and quiet
What to stop doing (common traps)
- Clock‑watching
- “Trying harder” to sleep
- Long naps to compensate
- Spending excessive time in bed awake
A simple 7‑day starter plan
1) Track a basic sleep diary for 7 nights (bedtime, wake time, awakenings).
2) Pick one consistent wake time and stick to it all week.
3) Get 10–20 minutes of outdoor light in the morning if possible.
4) Stop clock‑checking at night (turn the clock away).
5) Avoid long daytime naps; if you nap, keep it short and earlier.
Note: Small, steady habits plus CBT‑I skills create the conditions for deeper, more reliable sleep.
FAQs About Sleep Studies for Insomnia
Can a sleep study show insomnia?
A sleep study can show sleep fragmentation and arousals and help rule in/out other disorders, but insomnia is usually diagnosed clinically using symptoms and sleep patterns.
What if I can’t sleep during the test?
It’s common to sleep differently in a lab. Even partial sleep can provide useful data. Let the sleep team know if you’re anxious.
Is a home sleep test enough if I have insomnia?
HSAT is usually used when sleep apnea is suspected. For insomnia‑only concerns, testing may not be necessary—or an in‑lab study may be more informative if another disorder is suspected.
Are wearables accurate enough to replace a sleep study?
Wearables are useful for trends, but they can misclassify quiet wakefulness and don’t capture the full detail of PSG. Review (2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
What is the best treatment for chronic insomnia?
CBT‑I is first‑line, and digital/eHealth CBT‑I has meaningful evidence of benefit for many people. (JMIR 2024) https://mental.jmir.org/2024/1/e58217/
Note: Use testing to answer a specific question; use CBT‑I to address the insomnia pattern itself.
When to See a Sleep Specialist (or ENT/Sleep Team)
Consider a sleep evaluation if:
- you have loud snoring with choking/gasping or witnessed pauses in breathing,
- you experience significant daytime sleepiness or drowsy driving risk,
- you have unusual nighttime behaviors (parasomnias),
- insomnia lasts longer than 3 months or significantly affects daily life.
Tip: bring a 1–2 week sleep diary to your visit—it often speeds up the diagnostic process and helps determine whether a sleep study is likely to add value.
If you’d like to explore care with our team or get clarity on whether testing could help, you can request an appointment here: https://www.sleepandsinuscenters.com/
Note: If symptoms point to another sleep disorder or your insomnia isn’t improving, a specialist visit can help tailor next steps.
Conclusion — The Right Test + The Right Treatment Plan
A sleep study is not always required for insomnia, but it can be a powerful tool when symptoms suggest another sleep disorder, when insomnia persists despite high‑quality CBT‑I, or when the situation is clinically complex. For many people, the most effective next step is evidence‑based treatment—especially CBT‑I—plus identification and management of any contributing sleep or breathing disorders.
Note: Match the test to the question, and build treatment around proven skills that retrain sleep.
Medical Disclaimer
This article is for general educational purposes only and is not a substitute for medical advice, diagnosis, or treatment. If you have concerning symptoms (such as drowsy driving, witnessed breathing pauses, or dangerous nighttime behaviors), seek prompt care from a qualified clinician.
Sources
- American Academy of Sleep Medicine (AASM). Combination treatment for chronic insomnia guidance. https://aasm.org/combination-treatment-chronic-insomnia-guideline
- JMIR Mental Health (2024). Efficacy of eHealth versus In‑Person CBT‑I: Systematic Review and Meta‑Analysis of Equivalence. https://mental.jmir.org/2024/1/e58217/
- Polysomnography in Transition: Reassessing Its Role in the Future of Sleep Medicine (2025). https://pmc.ncbi.nlm.nih.gov/articles/PMC12592812/
- Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia: Meta‑Analysis of RCTs (2025). https://pmc.ncbi.nlm.nih.gov/articles/PMC12965280/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.