Sleep Apnoea and High Blood Pressure: Causes, Risks, and Treatment
Obstructive sleep apnoea (OSA) is common, often underdiagnosed, and closely linked with hypertension. For many people, sleep apnoea and high blood pressure show up together—sometimes because OSA can contribute to rising blood pressure over time, and sometimes because it can make blood pressure harder to control, including treatment-resistant hypertension. Research helps explain why this happens: repeated breathing interruptions can trigger nighttime stress signals in the body that push blood pressure up. [1]
A helpful way to picture it: each time the airway collapses, the body reacts like it’s hitting a small alarm—oxygen dips, sleep gets disrupted, and blood pressure can surge. When that repeats dozens of times per hour, night after night, those surges can start to show up in daytime blood pressure too. [1]
The encouraging part: treating OSA—often with CPAP—can improve blood pressure for many patients, and in pooled trials, CPAP plus structured weight-loss programmes lowered systolic blood pressure more than CPAP alone. [2][4]
Quick Summary (for skimmers)
The 30-second takeaway
- OSA is strongly linked to both having hypertension now and developing it later. [1]
- OSA is associated with about 2.8 times higher odds of treatment-resistant hypertension. [1]
- CPAP lowers systolic blood pressure modestly on average (~2–3 mmHg), with bigger drops in severe OSA, resistant hypertension, and good adherence (often around 4 hours or more per night). [2]
- CPAP plus structured weight loss can reduce systolic blood pressure more than CPAP alone in pooled trials (about ~8 mmHg). [4]

What Is Obstructive Sleep Apnoea (OSA)?
OSA vs. just snoring: OSA happens when the upper airway repeatedly narrows or collapses during sleep. That can cause breathing pauses (apnoeas), shallow breathing (hypopnoeas), drops in oxygen levels, and frequent brief awakenings that fragment sleep.
Snoring can be a sign of OSA—but not everyone who snores has OSA, and not everyone with OSA snores loudly. Some patients are surprised by their diagnosis because the biggest symptom they notice is stubborn fatigue or blood pressure that won’t cooperate.
Common terms you’ll see in testing: A key number on a sleep study is the AHI (apnoea–hypopnoea index)—the average number of breathing events per hour of sleep:
- Mild: 5–14
- Moderate: 15–29
- Severe: 30+
If you’d like a deeper explanation of severity categories and what they mean, see our guide: AHI score explained: understanding your sleep apnoea severity (https://sleepandsinuscenters.com/blog/ahi-score-explained-understanding-your-sleep-apnea-severity).
Bottom line: OSA is more than snoring—it’s repeated airway collapse that disrupts sleep and strains the cardiovascular system.
How Sleep Apnoea Raises Blood Pressure (The Why Behind the Link)
When people search sleep apnoea and high blood pressure, they’re often asking: How can something happening during sleep affect my blood pressure all day? The connection is real—and it’s not just one pathway, but several working together. [1]
Nighttime oxygen drops trigger a stress response: In OSA, breathing pauses can cause repeated oxygen dips—often called intermittent hypoxia. Your body responds as if it’s under threat, activating fight-or-flight (sympathetic) signals. Over time, these repeated surges can contribute to higher blood pressure and more strain on the cardiovascular system. [1]
A clinician might describe it simply: Your airway is closed, so your body tries to rescue you—heart rate and blood pressure jump, and sleep gets interrupted.
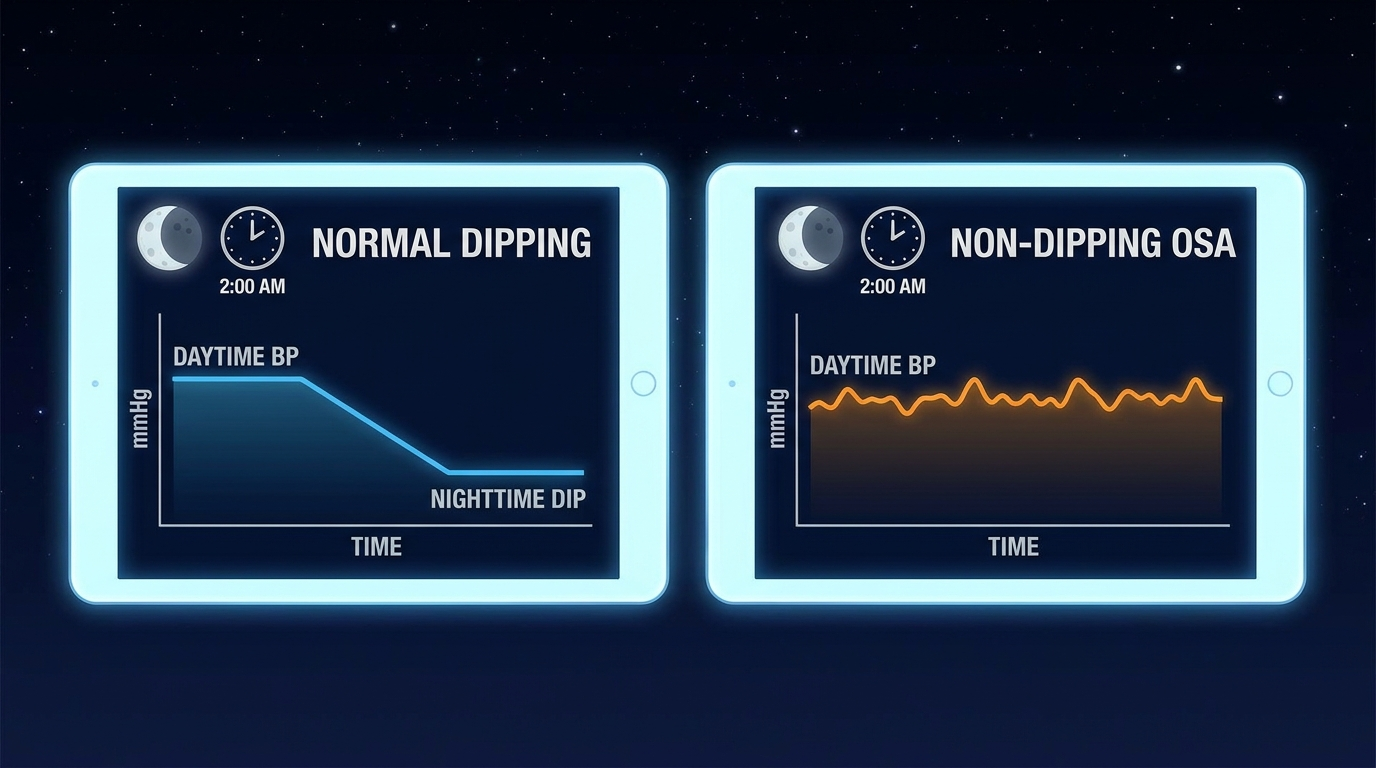
Blood pressure spikes during sleep—and the normal dip can disappear: Normally, blood pressure falls at night (a healthy dip). With OSA, the body may experience repeated blood pressure spikes during sleep, and some people develop a non-dipping blood pressure pattern—meaning their blood pressure stays relatively high overnight. Non-dipping patterns are associated with higher cardiovascular risk and can be an important clue that sleep-disordered breathing is in the picture. [1]
Concrete example: If someone wears a 24-hour ambulatory blood pressure monitor, a typical pattern is lower readings overnight. In OSA, those overnight readings may stay elevated—or jump repeatedly—despite normal daytime numbers.
Other pathways that keep BP elevated over time: OSA can influence blood pressure regulation in multiple ways, including:
- Repeated sympathetic surges and changes in chemoreflex/baroreflex function (how the body senses oxygen and pressure) [1]
- Large intrathoracic pressure swings (extra mechanical strain during obstructed breathing) [1]
- Inflammation and endothelial dysfunction (effects on blood vessel health) [1]
Takeaway: Repeated oxygen drops and arousals drive sympathetic surges and blunt normal nighttime BP dipping—key reasons OSA and hypertension often travel together.
Symptoms: When to Suspect Sleep Apnoea (Especially if You Have High BP)
Nighttime symptoms (often noticed by a partner):
- Loud, persistent snoring
- Choking/gasping sounds
- Witnessed pauses in breathing
- Restless sleep or frequent awakenings
- Nighttime urination
Daytime symptoms:
- Morning headaches
- Dry mouth on waking
- Fatigue, sleepiness, brain fog
- Irritability or mood changes
- Poor concentration
Blood-pressure clues that should raise suspicion:
- Resistant hypertension (blood pressure remains above goal despite three medications, typically including a diuretic)
- High morning readings
- Non-dipping patterns on ambulatory blood pressure monitoring
- Hypertension plus obesity or large neck circumference (risk factors often cluster together) [1]
Real-world pattern clinicians hear: I’m on multiple blood pressure pills and my readings are still high—especially in the morning. That combination often prompts an OSA evaluation.
If blood pressure is hard to control—especially with morning surges—consider OSA as a contributor worth evaluating.
Risks: Why the OSA–Hypertension Combination Is a Big Deal
Higher risk of developing hypertension and keeping it: OSA is associated with both prevalent hypertension (already present) and incident hypertension (developing later). It’s linked with having high blood pressure now and with higher odds of developing it over time. [1]
Resistant hypertension risk is much higher: OSA is associated with about 2.8 times higher odds of treatment-resistant hypertension. This is one reason clinicians often think about OSA when blood pressure stays high despite appropriate medication therapy. [1]
Cardiovascular complications to discuss with your clinician: Studies associate OSA with increased risk of conditions such as stroke, coronary artery disease, and certain heart rhythm issues. [1] This isn’t a prediction of what will happen to any one person—but it’s a strong reason to identify and treat contributing factors early.
Because OSA can sustain or worsen high BP and is linked with cardiovascular events, early recognition and treatment matter.
Who Should Be Screened for OSA if They Have High Blood Pressure?
High-priority groups:
- Resistant hypertension
- Obesity or metabolic syndrome
- Loud snoring plus daytime sleepiness
- Atrial fibrillation or other cardiovascular conditions (OSA screening is commonly considered in practice) [1]
Simple screening tools (not a diagnosis):
- STOP-BANG-style questions (Snoring, Tired, Observed apnoea, Pressure, BMI, Age, Neck, Gender)
- Epworth Sleepiness Scale (measures daytime sleepiness)
If you want to understand how daytime sleepiness is scored, see: Epworth Sleepiness Scale: a complete guide to understanding daytime sleepiness (https://sleepandsinuscenters.com/blog/epworth-sleepiness-scale-a-complete-guide-to-understanding-daytime-sleepiness).
If you have resistant hypertension or loud snoring with sleepiness, screening for OSA is a sensible next step.
Diagnosis: How Sleep Apnoea Is Confirmed
Home sleep test vs. in-lab sleep study: Many patients can be evaluated using a home sleep test, which typically measures airflow, breathing effort, oxygen levels, and heart rate. Home testing is often a good fit when there’s a strong suspicion of uncomplicated OSA.
An in-lab sleep study may be recommended in more complex situations—such as concern for other sleep disorders, certain cardiopulmonary conditions, or when home testing is inconclusive.
To learn more about choosing a test, visit: Home sleep test vs. lab study—Which sleep test is best for you? (https://sleepandsinuscenters.com/blog/home-sleep-test-vs-lab-study-which-sleep-test-is-best-for-you) You can also read about home sleep test accuracy (https://sleepandsinuscenters.com/blog/home-sleep-test-accuracy-how-reliable-are-at-home-sleep-tests).
What results matter for blood pressure risk: Beyond AHI, clinicians may also consider:
- Oxygen desaturation burden (how low and how often oxygen drops)
- Arousal frequency (how often sleep is disrupted)
These factors help explain why two people with similar AHI scores can experience different daytime symptoms—or different cardiovascular strain.
Confirming OSA—and quantifying oxygen drops and arousals—helps tailor treatment and set realistic blood pressure expectations.
Treatment: What Actually Helps Blood Pressure When You Treat OSA?
This is the practical heart of sleep apnoea and high blood pressure care: reducing airway collapse and the body’s nighttime stress response, while also addressing contributing risk factors like weight. [1]
CPAP therapy (first-line for many patients): CPAP (Continuous Positive Airway Pressure) helps keep the airway open, reducing breathing interruptions, oxygen drops, and sleep fragmentation—key drivers of nighttime blood pressure surges. [1]
Expected BP impact: Across studies, CPAP lowers systolic blood pressure by about 2–3 mmHg on average. [2]
Who tends to benefit more: People with severe OSA, resistant hypertension, and those who use CPAP consistently. [2]
Adherence matters: Better blood pressure improvements are often seen with more consistent nightly use, commonly around 4 hours or more per night. [2]
A practical note: Modest on average doesn’t mean not worth it. Some people see more meaningful changes, and CPAP can also improve sleep quality and daytime function by reducing breathing events. Your clinician can help set expectations based on your severity and blood pressure pattern.
To explore treatment options and what to expect, see our service page: Snoring & Sleep Apnoea Treatment (https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment).
Weight loss (especially when combined with CPAP): Weight can influence OSA by increasing airway narrowing and increasing physiological strain that supports higher blood pressure. Sustainable weight reduction can improve OSA severity for many patients and supports overall cardiovascular health.
Importantly, evidence suggests CPAP plus structured weight-loss programmes can reduce systolic blood pressure more than CPAP alone—around 8 mmHg pooled difference in clinical trials, though individual results vary. [4] In practice, that often looks like treating the airway obstruction and addressing the underlying drivers that make obstruction and hypertension more likely to persist.
Related reading: Sleep Apnoea and Weight Loss (ENT Perspective) (https://sleepandsinuscenters.com/blog/sleep-apnea-and-weight-loss-ent-perspective).
Other OSA treatments (where they may fit): Depending on anatomy, severity, and treatment preferences, other options may be considered:
- Oral appliance therapy: may help mild–moderate OSA or CPAP-intolerant patients
- Positional therapy: may help position-dependent OSA
- Learn more: Effective positional therapy for mild sleep apnoea (https://sleepandsinuscenters.com/blog/effective-positional-therapy-for-mild-sleep-apnea-a-comprehensive-guide)
- Surgical options: for selected cases with anatomy-driven obstruction
- Nasal/ENT optimisation: improving nasal airflow can make CPAP more comfortable and easier to use consistently
Blood pressure treatment still matters (OSA care is complementary): Treating OSA can support healthier blood pressure—but it’s generally considered complementary to a blood pressure plan guided by your clinician. This is especially relevant in obstructive sleep apnoea hypertension and resistant hypertension sleep apnoea situations, where a combined strategy is often needed. [1]
Treat the airway and the risk factors: CPAP plus weight management often yields the best blood pressure gains, alongside your regular BP plan.
Lifestyle Tips That Support Both Better Sleep and Lower Blood Pressure
Sleep-position and bedtime habits:
- Side sleeping can help some people with position-dependent OSA
- Keep a consistent sleep schedule when possible
- Avoid alcohol close to bedtime (it can worsen airway collapse)
Heart-healthy basics that also help OSA:
- Gradual, sustainable weight management
- Regular physical activity
- Sodium moderation and balanced eating patterns (DASH/Mediterranean-style principles)
CPAP success tips (to get the BP benefit): Comfort and consistency often drive results—especially when the goal is improving CPAP blood pressure response. [2] Helpful factors can include mask fit, humidification, and addressing nasal congestion and leaks.
If congestion is a barrier, see: Blocked nose during CPAP: ENT strategies (https://sleepandsinuscenters.com/blog/blocked-nose-during-cpap-ent-strategies).
Small, sustainable habit changes plus comfortable CPAP use can meaningfully support blood pressure control.
FAQs
Can sleep apnoea cause high blood pressure? Yes. OSA is strongly associated with developing and maintaining hypertension, largely through oxygen drops and repeated stress-response activation during sleep. [1]
Why is my blood pressure higher in the morning? OSA can cause nighttime blood pressure surges and reduce the normal overnight dip, which may contribute to higher morning readings. Non-dipping blood pressure patterns are common in OSA. [1]
Will CPAP cure my high blood pressure? CPAP typically lowers blood pressure modestly (~2–3 mmHg on average), but some people—especially those with severe OSA or resistant hypertension—may see larger improvements, particularly with consistent use. [2]
How many hours a night should I use CPAP to help blood pressure? Many studies show better blood pressure response with more consistent nightly use, commonly around 4 hours or more per night. [2]
Is weight loss or CPAP better for blood pressure? For many patients, the combination can be most effective. Trials suggest CPAP plus structured weight-loss programmes can lower systolic blood pressure more than CPAP alone (around ~8 mmHg pooled difference), though results vary. [4]
Who should get tested for sleep apnoea if they have hypertension? Testing is especially important for people with resistant hypertension, obesity, loud snoring, or excessive daytime sleepiness. [1]
When to See a Specialist (and What to Ask)
Signs you should book an evaluation: Consider an evaluation if you notice patterns commonly linked with sleep apnoea and high blood pressure, such as:
- Resistant hypertension
- Witnessed apnoeas, choking/gasping at night, or severe daytime sleepiness
- Persistent morning headaches or blood pressure that remains difficult to control
Questions to bring to your appointment:
- Should I be screened for OSA given my blood pressure pattern?
- Would a home sleep test be appropriate for me?
- What’s a realistic blood pressure change with CPAP in my case?
- Can you recommend a structured weight-loss approach alongside CPAP?
For a deeper overview of how these conditions interact, read: Sleep Apnoea and High Blood Pressure: The Connection (https://sleepandsinuscenters.com/blog/sleep-apnea-and-high-blood-pressure-the-connection).
If your blood pressure remains high despite treatment, a sleep evaluation can reveal a fixable contributor.
Conclusion
OSA is a common, treatable contributor to hypertension—especially resistant hypertension. The science behind the connection is well established: intermittent oxygen drops, sympathetic activation, and disrupted nighttime blood pressure patterns can all play a role. [1] While CPAP often lowers blood pressure modestly on average, the benefit can be more meaningful in severe OSA, resistant hypertension, and with consistent use—and combining CPAP with structured weight loss tends to produce the greatest blood pressure improvements. [2][4]
If you’re concerned about sleep apnoea and high blood pressure, book an appointment with Sleep and Sinus Centers of Georgia to discuss screening, testing options, and a treatment plan tailored to your anatomy, symptoms, and blood pressure goals: https://www.sleepandsinuscenters.com/
Citations
[1] Obstructive Sleep Apnoea and Hypertension: Critical Overview (2024). https://pmc.ncbi.nlm.nih.gov/articles/PMC11293186/
[2] Effect of CPAP on Blood Pressure in Obstructive Sleep Apnoea (2019). https://pmc.ncbi.nlm.nih.gov/articles/PMC7188383/
[3] Meta-analysis of CPAP on Cardiovascular Outcomes (2021). https://pmc.ncbi.nlm.nih.gov/articles/PMC9099124/
[4] Combined CPAP and Weight-Loss Therapy Improves Blood Pressure (2022). https://pmc.ncbi.nlm.nih.gov/articles/PMC10978146/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.