Is Narcolepsy Genetic? Causes, Heredity, and Risk Factors
Feeling overwhelmingly sleepy during the day—or noticing sudden muscle weakness with laughter or surprise—can be scary, especially if someone in the family has similar symptoms. It’s very common to wonder: Is narcolepsy genetic, and if so, what does that mean for your own risk (or your child’s)?
Below is a patient-friendly guide to what research shows about genes, immune triggers, and the underlying brain biology of narcolepsy—plus what typically happens during evaluation and treatment. The goal is clarity without alarm: narcolepsy can be disruptive, but it is often recognizable and treatable with appropriate care.
Quick Answer—Is Narcolepsy Genetic?
The short version
Narcolepsy—especially narcolepsy type 1 (NT1)—has a clear genetic risk component, but it usually does not follow a simple “passed down” inheritance pattern like some single-gene conditions. Most people who carry key risk genes never develop narcolepsy, which strongly suggests that genes plus environmental/immune triggers matter. (Nature, 2019; PNAS, 2019: https://www.nature.com/articles/s41439-018-0033-7, https://www.pnas.org/doi/10.1073/pnas.1818150116)
Genes may increase susceptibility, but they usually do not determine disease on their own.
Why people ask this question
— Symptoms like severe sleepiness can appear to “cluster” in families.
— Many people want clarity on children’s risk.
— People often hear about the HLA-DQB1*06:02 narcolepsy link and wonder whether genetic testing is helpful.
Bottom line: Genetics can raise risk, but most carriers never develop narcolepsy.
Narcolepsy Basics (Patient-Friendly Overview)
What narcolepsy is
Narcolepsy is a chronic neurological disorder that affects sleep-wake regulation. It’s best known for excessive daytime sleepiness (EDS) and REM sleep instability (for example, REM features appearing at unusual times). (Cleveland Clinic, 2025: https://my.clevelandclinic.org/health/diseases/12147-narcolepsy)
People sometimes describe EDS as “my brain feels pulled into sleep even when I’m trying,” not simply feeling tired after a late night.
If daytime sleepiness is hard to gauge, tools like the Epworth Sleepiness Scale (ESS) can help quantify it. Sleep and Sinus Centers of Georgia has a helpful guide: https://sleepandsinuscenters.com/blog/epworth-sleepiness-scale-a-complete-guide-to-understanding-daytime-sleepiness
Narcolepsy type 1 vs. type 2 (why the distinction matters for genetics)
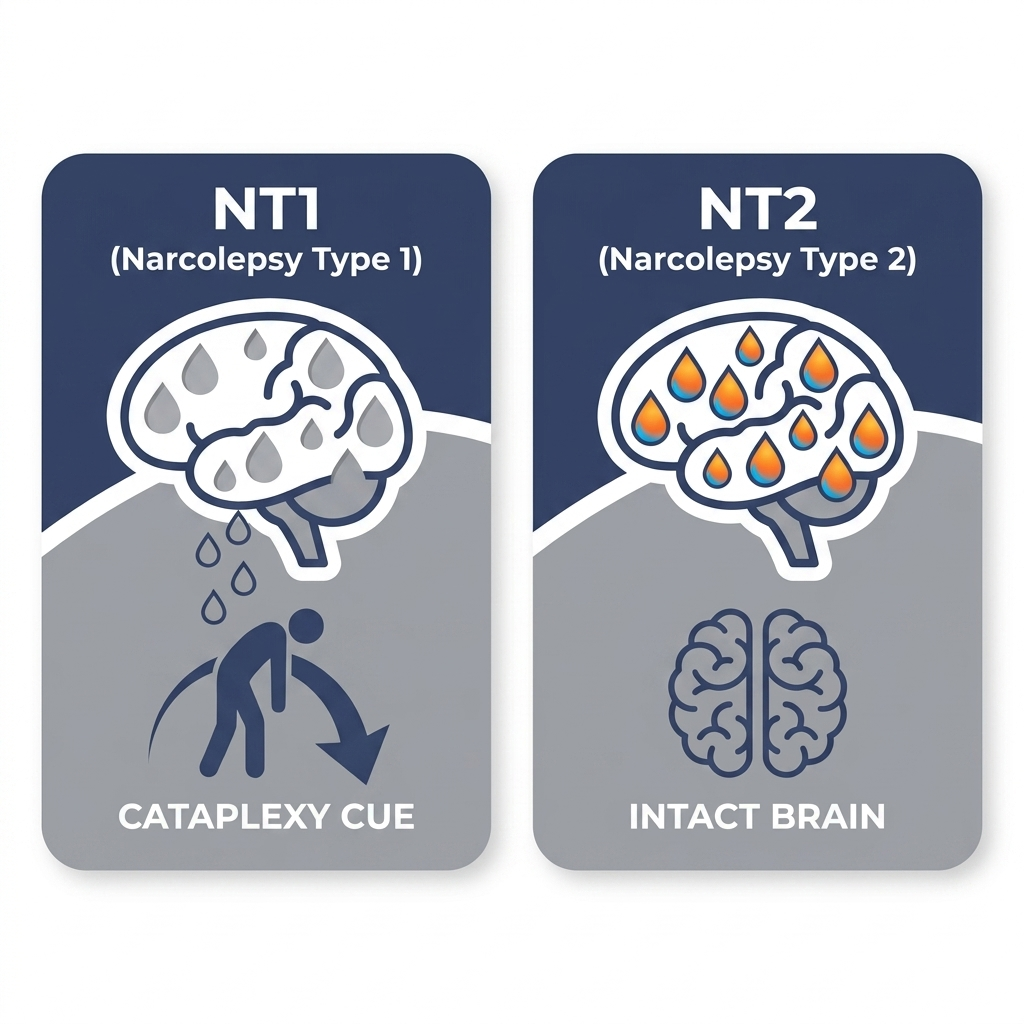
Understanding narcolepsy type 1 (NT1) vs. narcolepsy type 2 (NT2) is important because the “why” behind each type isn’t identical—and that difference shapes what we can (and can’t) say about heredity.
Narcolepsy type 1 (NT1): EDS plus cataplexy (sudden episodes of muscle weakness) and/or very low levels of hypocretin/orexin in the brain. NT1 has the strongest genetic and immune associations. (Nature, 2019; Cleveland Clinic, 2025)
Narcolepsy type 2 (NT2): EDS without cataplexy. NT2 appears more biologically diverse, and its genetic signals tend to be weaker/less consistent. (Nature, 2019)
In short: NT1 shows clearer immune-genetic patterns than NT2, which appears more heterogeneous.
Symptoms: What Narcolepsy Can Look Like Day-to-Day
Core symptoms
— Excessive daytime sleepiness (including “sleep attacks” or irresistible naps)
— Non-restorative sleep and frequent night awakenings (even though daytime sleepiness is prominent)
(Cleveland Clinic, 2025)
A concrete example: someone may sleep a full night yet still doze off during quiet moments—like reading, sitting in meetings, riding as a passenger in a car, or watching TV.
If persistent sleepiness is a concern, Sleep and Sinus Centers of Georgia offers a simple next step to help people self-screen: take our sleepiness test: https://sleepandsinuscenters.com/test-your-sleepiness
NT1 hallmark symptoms
— Cataplexy: brief loss of muscle tone triggered by emotion (often laughter, surprise, or excitement)
— Sleep paralysis
— Hypnagogic/hypnopompic hallucinations (dreamlike experiences when falling asleep or waking)
(Cleveland Clinic, 2025; hypocretin/orexin review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9371724/)
Cataplexy can look subtle or dramatic. Some people describe it as: “When I laugh hard, my knees wobble and my face feels slack for a few seconds.” Others may briefly drop objects, slump in a chair, or—less commonly—collapse while remaining conscious.
Symptoms that are often mistaken for something else
— ADHD-like inattention
— Depression or anxiety
— “Burnout”
— Medication side effects
— Sleep apnea or chronic insufficient sleep
This overlap is one reason people can go a long time without the right label—especially if the main complaint is “I can’t stay awake,” rather than a classic cataplexy story.
When symptoms should prompt evaluation
— Sleepiness affects safety (for example, driving) or performance at work/school
— Episodes strongly resemble cataplexy
If excessive sleepiness or possible cataplexy affects daily life or safety, a formal evaluation is warranted.

What Causes Narcolepsy in the Brain?
The key biology in NT1—loss of hypocretin/orexin neurons
The leading theory for NT1 is the loss of hypocretin (orexin)-producing neurons in the lateral hypothalamus. Hypocretin/orexin helps stabilize wakefulness and regulate REM sleep. When those neurons are lost, the result can be EDS, cataplexy, and REM “instability.” (Review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9371724/; additional background: https://pmc.ncbi.nlm.nih.gov/articles/PMC4028550/)
If you like analogies, hypocretin/orexin is often described as part of the brain’s “wake-stabilizing system.” When it’s missing, the boundary between wake and REM sleep can become leaky—so REM-like features can show up at the wrong time.
This is why many summaries describe NT1 using the phrase causes of narcolepsy (hypocretin/orexin deficiency)—it points to a core mechanism, not just a symptom.
Why NT2 is different
NT2 typically does not show the same clear hypocretin/orexin deficiency pattern. That’s one reason NT2 is often described as more heterogeneous (and why its genetics are less straightforward). (Nature, 2019)
NT1 centers on hypocretin/orexin loss; NT2 does not consistently show that same pattern.
The Genetic Link—What We Know (and What We Don’t)
The strongest known genetic risk factor: HLA-DQB1*06:02
When people ask “Is narcolepsy hereditary?”, they often run into one specific gene marker: HLA-DQB1*06:02.
HLA genes help the immune system distinguish “self” from “non-self.” Research shows HLA-DQB1*06:02 is strongly associated with increased NT1 risk—particularly NT1 with cataplexy. Importantly, it’s not destiny: many people with HLA-DQB1*06:02 do not have narcolepsy. (Nature, 2019; PNAS, 2019)
A brief clinician-style way of putting it: “HLA can be a useful clue—but it’s not a diagnosis.”
Narcolepsy is polygenic (not a single-gene “inherited disease”)
Current evidence supports narcolepsy—especially NT1—as a polygenic condition, meaning multiple genes (many tied to immune pathways) contribute to risk rather than one “narcolepsy gene” causing disease in a predictable way. (Nature, 2019)
A simple analogy: instead of one on/off switch, polygenic risk is more like multiple dimmer switches that together influence susceptibility.
Other immune-gene variants
Large genetic studies (GWAS) also point toward additional immune-related signals beyond HLA—again suggesting immune regulation plays a central role in susceptibility. (PNAS, 2019)
If it’s genetic, why doesn’t everyone in my family have it?
This is where the idea of low penetrance helps: a person can carry risk genes, but without the right combination of immune/environmental factors, narcolepsy may never develop. Different family members can share genes—but not share the same triggers or immune events.
Think “increased susceptibility,” not certainty—many carriers never develop narcolepsy.
Autoimmune Connection—Why Genes Alone Aren’t Enough
The leading model: autoimmune attack in genetically susceptible people
A widely supported model is that NT1 involves an immune-mediated (autoimmune) process targeting hypocretin/orexin neurons in genetically susceptible individuals. (Nature, 2019; review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9371724/)
In other words, the same genetic signals that point to immune involvement also fit the core biology: the cells that make hypocretin/orexin are missing or severely reduced in NT1.
Hypocretin peptides as autoantigens (plain-language meaning)
Some research suggests hypocretin-related peptides may function as autoantigens—meaning the immune system may mistakenly treat part of the hypocretin/orexin system as a target. This helps explain why immune genetics (like HLA) are so relevant in NT1. (Autoantigen research, 2023: https://pmc.ncbi.nlm.nih.gov/articles/PMC12515106/)
“Autoantigen” can sound abstract, but the basic concept is straightforward: the immune system may confuse a normal protein fragment for something it needs to attack.
Environmental “triggers” that may start the immune process
Some studies have reported associations between narcolepsy and certain infections or vaccines in specific settings, but causation has not been established. The key point is careful wording: these are associations and appear to involve immune activation plus genetic susceptibility, not a universal cause-and-effect for everyone. (Nature, 2019)
The prevailing view: NT1 reflects immune dysregulation in susceptible people, sometimes after an immune-triggering event.
Is Narcolepsy Hereditary? Understanding Family Risk
What “runs in families” typically means
Research suggests first-degree relatives may have a higher risk than the general population, but narcolepsy remains uncommon overall. In practical terms, “runs in families” usually reflects shared susceptibility, not guaranteed inheritance. (Nature, 2019)
It can help to separate “this is more likely than average” from “this will happen.” Many families fall into the first category, not the second.
If a parent has NT1, what about children?
This is a helpful place to separate relative risk (higher than average) from absolute risk (still low in most families). For many families, the most useful approach is awareness: recognizing symptoms early if they appear—rather than assuming narcolepsy will occur. Keeping a short log of sleepiness patterns, naps, and any emotion-triggered weakness can make a future evaluation more efficient.
Should families get genetic testing (HLA testing)?
HLA-DQB1*06:02 testing cannot diagnose narcolepsy by itself and does not reliably predict who will develop it. In some clinical situations, it may be used as one piece of a broader evaluation—but it’s not a stand-alone answer to “Is narcolepsy genetic?” (Nature, 2019; Cleveland Clinic, 2025)
Family risk is generally low in absolute terms; awareness and timely evaluation matter more than screening tests.

Other Risk Factors That Can Increase the Odds
Age and typical onset
Narcolepsy often begins in childhood/adolescence or young adulthood, though it can be recognized later. Timing can matter because early symptoms may be mislabeled as “teen sleep habits,” stress, or mood issues.
Sleep deprivation and irregular schedules (not a cause, but can unmask symptoms)
Insufficient sleep and shifting schedules don’t cause narcolepsy, but they can worsen EDS and make underlying symptoms more obvious—adding extra sleep debt on top of an already unstable sleep-wake system.
Co-existing sleep disorders
Conditions such as sleep apnea, circadian rhythm disorders, and chronic insufficient sleep can mimic or worsen sleepiness—one reason a structured evaluation matters.
Risk factors can amplify symptoms, but they typically don’t cause narcolepsy on their own.
How Narcolepsy Is Diagnosed (What to Expect)
Start with a clinical history
A typical evaluation reviews how long EDS has been present, whether episodes sound like cataplexy, sleep schedule and sleep quality, and medications, substances, and mental health factors.
If you’re preparing for an appointment, it can help to bring specifics: “I nap every day at 2 p.m.,” “I’ve had two episodes of weakness when laughing,” or “I fall asleep within minutes during passive activities.”
Rule out more common causes of sleepiness
Clinicians often consider other contributors such as sleep apnea, medication effects, depression, and certain medical issues. This step matters because treating the “more common” causes can sometimes fully resolve symptoms—or reveal what’s left after they’re addressed.
Sleep testing
A common pathway is an overnight polysomnography (PSG) followed by a next-day MSLT (multiple sleep latency test). The MSLT measures how quickly someone falls asleep in quiet daytime nap opportunities and whether REM sleep appears unusually quickly (often described as “sleep-onset REM periods”). (Cleveland Clinic, 2025)
For a general overview of testing logistics, Sleep and Sinus Centers of Georgia explains home sleep test vs. in-lab sleep study: https://sleepandsinuscenters.com/blog/home-sleep-test-vs-lab-study-which-sleep-test-is-best-for-you —narcolepsy evaluations commonly rely on in-lab testing.
When hypocretin/orexin testing is used
In some scenarios, measuring hypocretin/orexin in cerebrospinal fluid (CSF) can support an NT1 diagnosis. (Review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9371724/)
A structured history plus targeted testing helps distinguish narcolepsy from more common causes of sleepiness.

Treatment Options (Symptoms Can Improve Significantly)
There’s no single “cure,” but symptoms are treatable
Narcolepsy is typically managed long-term using a personalized plan focused on symptoms and safety. (Cleveland Clinic, 2025)
Many patients find that the combination of the right medication plan plus consistent routines makes symptoms far more predictable—even if they don’t disappear completely.
Medications for excessive daytime sleepiness
Treatment commonly includes wake-promoting medications and/or stimulants, selected and monitored by a clinician based on response and side effects. (Cleveland Clinic, 2025)
Treatments for cataplexy and REM symptoms
Cataplexy and REM-related symptoms may be treated with REM-suppressing medications and clinician-managed options such as oxybate formulations. (Cleveland Clinic, 2025)
Safety planning
Because sleepiness can affect reaction time and attention, safety planning often includes strategies to reduce drowsy driving risk and to support functioning at work or school. For some people, even small changes—like scheduled naps and avoiding long late-day drives—can make a meaningful difference.
With appropriate care, many people achieve better symptom control and safer routines.
Lifestyle Tips That Actually Help (Alongside Medical Care)
— Consistent sleep schedule: stable sleep and wake times can reduce “extra” sleepiness layered on top of narcolepsy.
— Planned naps: short, scheduled naps may be more refreshing than unplanned sleep attacks for some people.
— Managing triggers: alcohol, sedating medications (only with clinician guidance), and sleep deprivation can worsen symptoms.
— Support at work/school: accommodations might include flexible breaks for brief naps, adjusted schedules, or testing supports.
— Mental health support: narcolepsy can overlap with anxiety/depression; screening and support groups can be valuable.
Small, consistent changes often add up—especially when paired with medical treatment.
FAQs
Can you have narcolepsy if no one in your family has it?
Yes. Many people diagnosed with narcolepsy report no known family history. Genetics can raise susceptibility, but family clustering isn’t required.
If I have the HLA-DQB1*06:02 gene, will I get narcolepsy?
Not necessarily. HLA-DQB1*06:02 is a risk factor, not a diagnosis. Many carriers never develop narcolepsy. (Nature, 2019; PNAS, 2019)
What’s the difference between narcolepsy and sleep apnea fatigue?
Sleep apnea-related fatigue often stems from breathing disruptions and fragmented sleep, while narcolepsy involves neurologic sleep-wake instability and may include features like cataplexy or REM intrusion symptoms. Testing helps distinguish them.
Is narcolepsy autoimmune?
Evidence strongly supports autoimmune involvement in narcolepsy type 1, with ongoing research into specific targets and immune mechanisms. (Nature, 2019; autoantigen research, 2023)
Can infections trigger narcolepsy?
Associations have been reported between certain infections and narcolepsy onset in genetically susceptible people. This does not mean infections cause narcolepsy in most people. (Nature, 2019)
Does narcolepsy get worse with age?
Symptoms can change over time. Some people report more stable patterns with treatment and routines, while others notice fluctuations. Follow-up and adjustment of management strategies can matter.
When should I see a sleep specialist?
When daytime sleepiness is persistent, affecting safety or daily life, or when episodes resemble cataplexy, a sleep evaluation can clarify next steps. For general triage guidance: https://sleepandsinuscenters.com/when-to-see-an-ent-for-sleep-problems
Implementation note: This FAQ section can be marked up with FAQPage schema to support rich results.
If symptoms are frequent or safety is a concern, a sleep specialist can help guide testing and treatment.
When to Seek Care (Next Steps)
In general, narcolepsy is worth evaluating when there are:
— Frequent uncontrollable sleep episodes
— Suspected cataplexy (emotion-triggered muscle weakness)
— Sleepiness affecting driving or workplace/school safety
Because several common conditions can mimic narcolepsy, formal history and sleep testing are often the most efficient way to get clarity rather than relying on self-diagnosis.
If you’re ready to talk with a sleep professional about symptoms, testing, or treatment options, you can book an appointment through Sleep and Sinus Centers of Georgia: https://www.sleepandsinuscenters.com/
Early evaluation can shorten the path to effective treatment and safer daily routines.
References
— Nature — Genetics of narcolepsy (2019): https://www.nature.com/articles/s41439-018-0033-7
— PNAS — Type 1 narcolepsy association study (2019): https://www.pnas.org/doi/10.1073/pnas.1818150116
— Cleveland Clinic — Narcolepsy overview (2025): https://my.clevelandclinic.org/health/diseases/12147-narcolepsy
— PMC — Hypocretin/orexin deficiency and NT1 (review): https://pmc.ncbi.nlm.nih.gov/articles/PMC9371724/
— PMC — Additional hypocretin/orexin/narcolepsy background: https://pmc.ncbi.nlm.nih.gov/articles/PMC4028550/
— PMC — Amidated hypocretin peptides as autoantigens (2023): https://pmc.ncbi.nlm.nih.gov/articles/PMC12515106/
Medical disclaimer
This article is for general education and is not a substitute for professional medical advice, diagnosis, or treatment. If you have symptoms such as unsafe sleepiness, possible cataplexy, or concerns about driving, seek care from a qualified clinician.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.