Hypnotic Medications: Uses, Side Effects, and Safety Tips
Quick Take—What This Article Covers
- What hypnotic medications are and when they’re used for insomnia
- Common insomnia symptoms and causes
- Treatment options (starting with non-medication approaches)
- Key medication classes—including newer dual orexin receptor antagonists (DORAs) like Dayvigo and Quviviq
- Side effects, warnings, interactions, and practical safety tips
- FAQs patients commonly ask in clinic
What Are Hypnotic Medications?
Hypnotics are medications designed to help with sleep onset (falling asleep), sleep maintenance (staying asleep), or both. They’re typically considered when insomnia is persistent and causes daytime impairment—like fatigue, poor focus, irritability, or mood changes.
A helpful way to think about it: hypnotic medications may “turn down the wake signal” enough to let sleep happen, but they don’t automatically fix why sleep became difficult in the first place.
Why “sleeping pills” aren’t one-size-fits-all
- Not all insomnia looks the same. Some people can’t fall asleep; others fall asleep but wake repeatedly or too early.
- Risks can vary by age, other health conditions, and other medications or supplements.
In clinic, a common comment is: “I don’t need to sleep 12 hours—I just need my brain to stop being ‘on’ at 2 a.m.” That difference matters when choosing a treatment plan.
*Bottom line: Hypnotics can reduce the brain’s wake drive, but a full plan also addresses the reasons sleep became hard in the first place.*

Insomnia Symptoms (When a Hypnotic Might Be Considered)
Nighttime symptoms
- Trouble falling asleep (sleep-onset insomnia)
- Trouble staying asleep (sleep-maintenance insomnia)
- Waking too early and not being able to fall back asleep
- Sleep that doesn’t feel restorative
Daytime symptoms linked to insomnia
- Fatigue, low energy, irritability
- Trouble focusing or “brain fog”
- Reduced performance at work/school, more mistakes
- Worry about sleep that can create a frustrating cycle
If daytime sleepiness is part of the picture, a quick screening tool like the Epworth Sleepiness Scale can help you quantify symptoms: https://sleepandsinuscenters.com/blog/epworth-sleepiness-scale-a-complete-guide-to-understanding-daytime-sleepiness
Practical note: If you’re consistently sleepy during the day, it’s worth asking whether something like sleep apnea or another sleep disorder is fragmenting sleep—because adding a hypnotic without addressing the driver can sometimes backfire.
*If daytime sleepiness is significant, screen for other sleep disorders so treatment targets the right problem.*
Common Causes of Insomnia (and Why This Matters for Medication Choice)
Medical and sleep-related contributors
- Sleep apnea (breathing interruptions can fragment sleep)
- Restless legs, chronic pain, reflux, nasal obstruction
- Frequent nighttime urination
- Side effects from certain medications (for example: stimulants, steroids, some antidepressants)
If sleep apnea is suspected, it’s often important to address it directly—learn more about snoring and sleep apnea treatment options here: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
Nasal breathing issues can also affect sleep quality. Here’s a helpful overview of nasal obstruction and insomnia: https://sleepandsinuscenters.com/blog/nasal-obstruction-and-insomnia-understanding-the-link-for-better-sleep
Why this changes the medication conversation
If breathing is disrupted at night, the goal isn’t just “more sleep”—it’s better-quality sleep. Clinicians often screen for sleep apnea before escalating hypnotic medications, especially when loud snoring, witnessed pauses, or significant daytime sleepiness are present.
Mental health and stress-related contributors
- Anxiety, depression, PTSD, grief, high stress
- Substance use (including alcohol, cannabis, sedatives)
Lifestyle / schedule contributors
- Shift work, travel/jet lag
- Late caffeine, late workouts, heavy evening meals
- Bright screens/phone use close to bedtime
Identifying the likely drivers matters because hypnotic medications may help symptoms, but they don’t always fix the underlying cause.
*Targeting root causes leads to more refreshing sleep than simply adding sedation.*
First-Line Treatment: Non-Medication Options (Often Recommended Even If You Use a Hypnotic)
Clinical practice often emphasizes cautious use of insomnia medications and behavioral treatment when appropriate.
CBT-I (Cognitive Behavioral Therapy for Insomnia)
- Stimulus control (retraining the bed/bedroom as a cue for sleep)
- Sleep restriction (compressing time in bed to rebuild stronger sleep drive)
- Cognitive tools (reducing unhelpful sleep worry)
- Relaxation strategies
A simple analogy: if insomnia has “trained” your brain that the bed is a place to be alert and anxious, CBT‑I helps “retrain” that association—so sleep becomes more automatic again.
Sleep hygiene basics that actually help
- Consistent wake time and a predictable wind-down routine
- A dark, quiet, cool sleep environment
- Better timing of caffeine/alcohol and evening meals
- Screen-light strategies at night
More on sleep hygiene here: https://sleepandsinuscenters.com/blog/sleep-hygiene-and-its-impact-on-ent-disorders-key-insights
*Skills-first approaches like CBT‑I often improve sleep more durably than pills alone.*

Treatment Options Overview (Where Hypnotics Fit)
The stepwise approach many clinicians use
1) Screen for other sleep disorders (especially sleep apnea)
2) Start with CBT-I plus targeted lifestyle changes
3) Consider short-term medication support when insomnia is severe or persistent
If testing is needed, this guide can help you understand home sleep test vs. lab sleep study options: https://sleepandsinuscenters.com/blog/home-sleep-test-vs-lab-study-which-sleep-test-is-best-for-you
Goals of medication therapy
- Improving sleep enough to restore daytime functioning
- Using the lowest effective dose for the shortest appropriate duration
- Reassessing regularly (rather than “set and forget” refills)
A clinician’s “success metric” is often less about a perfect sleep tracker score and more about: Are you safer, functioning better, and relying less on emergency fixes?
*Medication is one tool among many—clear goals and regular check-ins keep it safer and more effective.*

Main Types of Hypnotic Medications (Patient-Friendly Comparison)
Benzodiazepines
- Often used for: Sleep onset and/or maintenance issues
- Common side effects: Next-day grogginess, memory problems, dizziness
- Key cautions: Tolerance and dependence risk; falls/confusion in older adults
“Z-drugs” (nonbenzodiazepines)
- Often used for: Sleep onset; some agents also help maintenance
- Common side effects: Next-day impairment
- Key cautions: Risk of complex sleep behaviors; caution with other sedatives
Melatonin receptor agonists (such as ramelteon)
- Often used for: Circadian rhythm issues and some insomnia patterns
- Common side effects: Usually mild (headache, dizziness)
- Key cautions: Different from over-the-counter melatonin; quality and dosing vary
Off-label sedating medications (some antidepressants/antihistamines)
- Often used for: Situations where another medical need coexists
- Common side effects: Dry mouth, constipation, next-day sedation
- Key cautions: “Sedating” does not always mean better or healthier sleep; anticholinergic side effects may be problematic, especially in older adults
Clarifier: “Sedating” is not automatically the same as “improves healthy sleep.” Some medications make people drowsy but can still lead to grogginess, poor-quality sleep, or side effects that outweigh benefits.
*Choosing a sleep medicine is about matching symptoms and risks—not chasing sedation.*
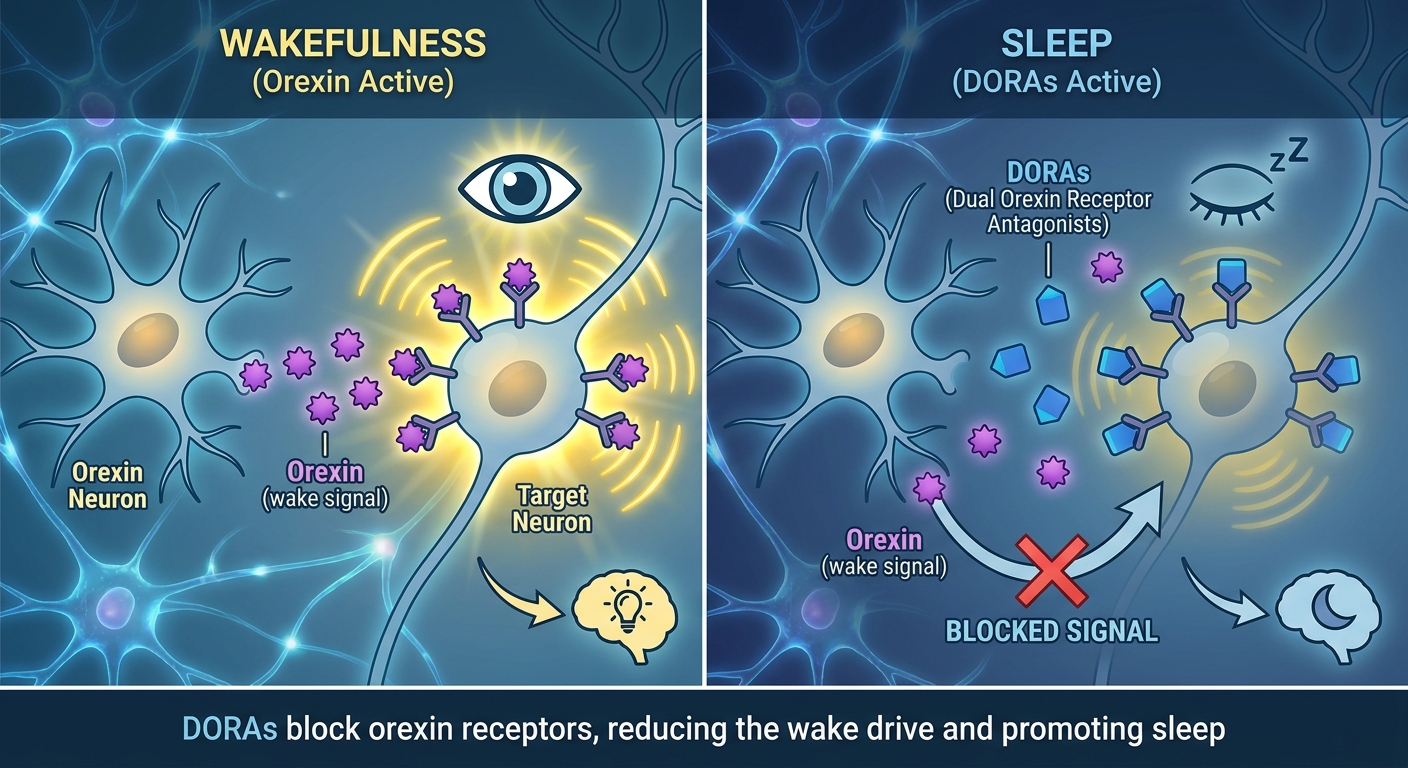
Newer Hypnotics: Dual Orexin Receptor Antagonists (DORAs)
Orexin is a brain signaling system that helps keep you awake and alert. DORAs work by blocking orexin signaling, which supports sleep in a different way than medications that broadly “sedate” the brain.
You can think of orexin like the brain’s “stay awake” messenger. DORAs don’t push sedation from the outside as much as they reduce that internal wake drive.
Examples and FDA-approved indications
- Lemborexant (Dayvigo) — FDA approval 2019; indicated for insomnia with sleep onset and/or maintenance difficulty [2]
- Daridorexant (Quviviq) — FDA approval 2022; indicated for insomnia with sleep onset and/or maintenance difficulty [3]
Typical dosing and timing basics (from prescribing information)
- Dayvigo (lemborexant): 5–10 mg [2]
- Quviviq (daridorexant): 25–50 mg [3]
Both are generally taken about 30 minutes before bedtime, and only when there is enough time for a full night of sleep (at least 7 hours), per labeling. [2][3]
That “time in bed” detail matters—many next-day problems happen when medicines are taken too late or when an early alarm shortens sleep opportunity.
What research says about effectiveness
Clinical trials and systematic reviews support DORAs as effective for both sleep onset and sleep maintenance. [4] A 2024 systematic review also highlights growing interest in DORAs for insomnia occurring alongside psychiatric comorbidities. [4]
How DORAs differ from benzodiazepines/Z-drugs
DORAs don’t work by directly enhancing the same calming pathways as benzodiazepines and many Z‑drugs. In studies, DORAs have not shown the same dependence/withdrawal pattern seen with some older sedative-hypnotics, but they still require careful use and have important warnings and interaction considerations. [2][3]
*DORAs reduce the wake signal rather than broadly sedating—an option with different benefits and cautions to review with your clinician.*
Side Effects and Safety Risks (Across Hypnotics—Including DORAs)
Next-day impairment
- Grogginess or “hangover” feeling
- Slower reaction time
- Reduced alertness
This matters for driving, operating equipment, and early-morning responsibilities. If you notice impairment, treat it as a safety issue and report it to your prescriber.
Complex sleep behaviors
- Sleepwalking
- Sleep-driving
- Preparing/eating food with little or no memory afterward
If a complex sleep behavior occurs, treat it as a serious warning and discuss promptly with the prescribing clinician. [2][3]
DORA-specific warning symptoms
- Sleep paralysis
- Hypnagogic/hypnopompic hallucinations
- Cataplexy-like symptoms (brief muscle weakness), sometimes with strong emotions [2][3]
CNS depressant effects and combining sedatives
Alcohol, opioids, benzodiazepines, and some antihistamines/anxiety medications can add sedation and increase impairment risk. [2][3]
Dependence, tolerance, and rebound insomnia
Risks vary by class. Some medicines are associated with tolerance/dependence, and abrupt discontinuation can cause rebound insomnia. Tapering is individualized.
*If safety concerns or unusual symptoms appear, pause high‑risk activities and contact your clinician promptly.*
Drug Interactions & Contraindications (Especially Important for DORAs)
CYP3A interactions
DORAs are affected by CYP3A. Some drugs can raise DORA levels (increasing side effects) or lower them (reducing effectiveness). Share a complete medication and supplement list with your clinician. [2][3]
A simple way to remember this: CYP3A interactions can change how much medication is “left in your system” by morning—affecting both benefit and next-day risk.
Contraindication: narcolepsy
DORAs should not be used in people with narcolepsy. [2][3]
Caution in certain health situations
- Older adults (falls, confusion, next-day impairment)
- Liver impairment (dose adjustments or avoidance may apply) [2][3]
*Review your full medication list and medical history with your prescriber before starting a hypnotic—interactions and contraindications matter.*
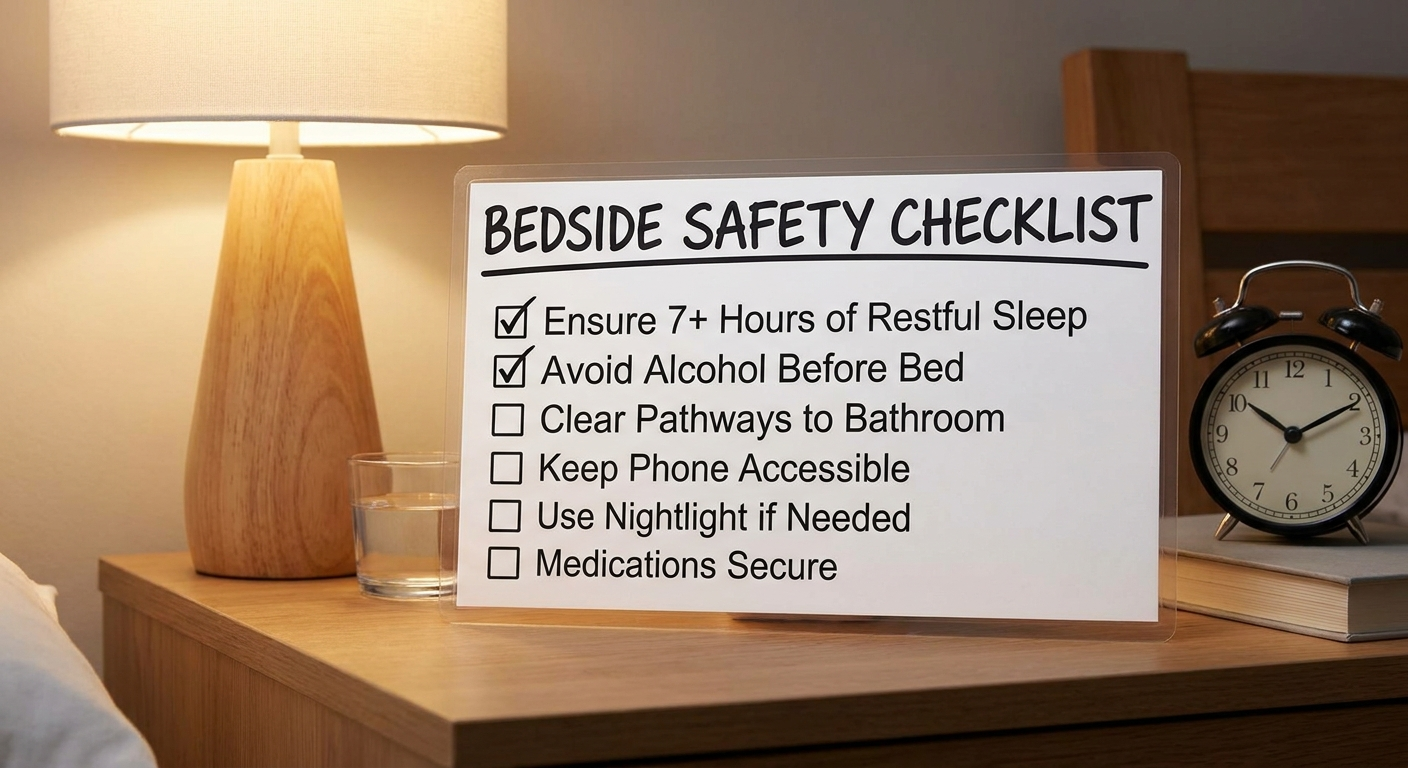
Safety Tips Checklist (Practical, Patient-Friendly)
Before starting a hypnotic
- Could something else be driving insomnia (sleep apnea, reflux, anxiety, medication effects)?
- Is CBT-I part of the plan? [1]
- Are there interacting sedatives or CYP3A-related interactions to review? [2][3]
How to take it more safely
- Use the lowest effective dose
- Take only when a full night of sleep is possible (at least 7 hours for DORAs) [2][3]
- Avoid alcohol and other sedatives unless specifically cleared by the prescriber [2][3]
- Avoid “double dosing” after nighttime awakenings unless specifically directed
Safety the next morning
- If you feel impaired, avoid driving and safety-sensitive tasks
- Be cautious with nighttime bathroom trips (balance and fall risk)
When to call the doctor urgently
- Confusion, fainting, or severe abnormal nighttime behaviors
- New or distressing hallucinations or sleep paralysis episodes
- Any complex sleep behavior event [2][3]
*Plan ahead for a full night’s sleep and treat next‑day grogginess as a safety signal, not a nuisance.*
When to See a Sleep Specialist (or ENT) Instead of Just Trying Another Pill
Consider evaluation if you have:
- Loud snoring, witnessed breathing pauses, waking up gasping
- Morning headaches, dry mouth, or high blood pressure
- Significant daytime sleepiness despite enough time in bed
This overview may help: When to see an ENT for sleep problems https://sleepandsinuscenters.com/blog/when-to-see-an-ent-for-sleep-problems
If you’ve had sleep apnea testing (or are considering it), understanding the sleep apnea severity (AHI) score can be useful: https://sleepandsinuscenters.com/blog/ahi-score-explained-understanding-your-sleep-apnea-severity
*If red flags for another sleep disorder are present, evaluation often improves outcomes more than switching to a different pill.*
FAQs (SEO-Friendly)
What’s the difference between sleep onset and sleep maintenance insomnia?
Sleep onset insomnia is difficulty falling asleep. Sleep maintenance insomnia is difficulty staying asleep (frequent awakenings or waking too early).
Are orexin receptor antagonists like Dayvigo or Quviviq addictive?
In clinical studies, DORAs have not shown the same dependence/withdrawal pattern seen with some older sedative-hypnotics, but they still carry meaningful risks, are prescription medications, and should be used with careful monitoring. [2][3]
Can I take hypnotic medications every night?
Some people use hypnotic medications short-term, while others may use them longer with periodic reassessment. Clinical practice often emphasizes cautious use and pairing medication with CBT-I when appropriate. [1]
What if I feel sleepy the next day?
Next-day impairment is a known risk with many sleep medicines. Treat that symptom as a safety issue (especially for driving) and discuss timing/dose options with the prescriber. [2][3]
Can I drink alcohol with sleep meds?
Alcohol can add to sedating effects and increase impairment risk. Many medication labels caution against combining alcohol with hypnotics. [2][3]
What medications interact with these sleep aids?
Interactions depend on the medication class. For DORAs, CYP3A interactions are especially important, and combining multiple sedatives can raise risk. [2][3]
Conclusion + Call to Action
Insomnia is common and treatable, but the safest plan is individualized. Non-medication approaches like CBT‑I often form the foundation, while hypnotic medications may be considered when symptoms are severe or persistent—especially after evaluating for underlying causes like sleep apnea or nasal obstruction.
If you’d like help with insomnia evaluation, sleep testing, or treatment planning, book an appointment with Sleep and Sinus Centers of Georgia here: https://sleepandsinuscenters.com/appointments
Learn more about the practice: https://www.sleepandsinuscenters.com/
*Effective insomnia care combines skill-building, smart evaluation, and the careful use of medication when needed.*
References
[1] American Academy of Sleep Medicine (AASM). Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults (2017). https://aasm.org/resources/pdf/pharmacologictreatmentofinsomnia.pdf
[2] Dayvigo (lemborexant) Prescribing Information (FDA, 2019). https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/212028s000lbl.pdf
[3] Quviviq (daridorexant) Prescribing Information (FDA, 2022). https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214985s000lbl.pdf
[4] Orexin receptor antagonists in the treatment of insomnia associated with psychiatric disorders: a systematic review (2024). https://pmc.ncbi.nlm.nih.gov/articles/PMC11401906/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.