Cure for Insomnia: Proven Treatments and Tips for Better Sleep
If you’re searching for a cure for insomnia, it helps to start with realistic expectations: there isn’t one single, universal fix that works for everyone. The encouraging part is that many people can achieve lasting improvement, and some may experience remission, when treatment addresses the main drivers of their insomnia.
Think of insomnia less like a single disease with a single antidote, and more like a stuck system: your schedule, stress response, habits in bed, and sometimes a medical issue can all keep the problem going. The most effective treatments often address the underlying patterns that keep insomnia going, rather than relying only on sedation.
In this guide, you’ll learn what insomnia is, when it becomes chronic, common symptoms and root causes, and the most evidence-based approaches to insomnia treatment—including CBT‑I (first-line by major guidelines) and newer medications like dual orexin receptor antagonists (DORAs). We’ll also cover practical strategies and FAQs. CBT‑I is widely recommended as the first-line approach for chronic insomnia [3][4].
— In short, lasting progress usually comes from treating the drivers of insomnia, not just the symptoms. —
What Is Insomnia (and When Does It Become “Chronic”)?
Insomnia is trouble falling asleep, staying asleep, or waking too early, along with daytime impairment (fatigue, concentration problems, mood changes, or reduced functioning). It’s not just a bad night—it shows up in your day.
Acute insomnia typically lasts days to weeks and is often linked to stress, illness, travel, or schedule disruption. Chronic insomnia is a persistent pattern lasting at least 3 months and frequent enough to affect daytime life. Acute might be a rough week after travel; chronic feels baked in, and worry about sleep becomes part of the problem.
Insomnia matters for health and quality of life: ongoing poor sleep impacts mood, memory, productivity, and safety (including drowsy driving), and can worsen other health issues over time. Many people describe the uncertainty—will tonight be another struggle?—as the hardest part.
— Bottom line: insomnia affects both nights and days, so it’s worth addressing early and thoughtfully. —
Insomnia Symptoms (Nighttime + Daytime)
Common nighttime symptoms include taking a long time to fall asleep, waking often, waking too early and being unable to return to sleep, and sleep that feels light or non-restorative. Common daytime symptoms include fatigue or low energy, irritability or low mood, brain fog and reduced concentration, and worry about sleep (which can worsen sleep).
A simple way to tell insomnia from just not enough sleep: if you have time for sleep but can’t consistently get it or keep it, insomnia may be in the mix.
When symptoms might signal something else: loud snoring, choking, or gasping during sleep; uncomfortable leg sensations with an urge to move; panic-like awakenings; medication or substance effects (including stimulants or alcohol timing); or symptoms that persist or worsen despite basic changes. If these persist, consider a clinical evaluation to clarify the root cause.
What Causes Insomnia? (The Most Common Root Issues)
Stress, anxiety, and hyperarousal are common drivers: a wired-but-tired state, racing thoughts, physical tension, or a learned pattern of being awake in bed. Over time, the brain can associate the bed with wakefulness, problem-solving, clock-checking, or frustration—exactly when you want the opposite.
Sleep schedule and circadian rhythm mismatches also matter: shift work, irregular schedules, sleeping in on weekends, and late-night bright light can push the body clock later. Even small shifts count; if your wake time swings by 2–3 hours across the week, your rhythm may never fully stabilize.
Medical contributors are often overlooked: sleep-disordered breathing (including sleep apnea), chronic pain, reflux, menopause-related hot flashes, thyroid problems, and nasal blockage or congestion can fragment sleep. If nasal breathing is difficult at night, this can be meaningful. Overview on nasal obstruction and insomnia: https://sleepandsinuscenters.com/blog/nasal-obstruction-and-insomnia-understanding-the-link-for-better-sleep
Medications, caffeine, alcohol, and nicotine can also disrupt sleep—especially later in the day. Alcohol may help you fall asleep but often worsens middle-of-the-night awakenings; a no-alcohol-close-to-bed test is often revealing.
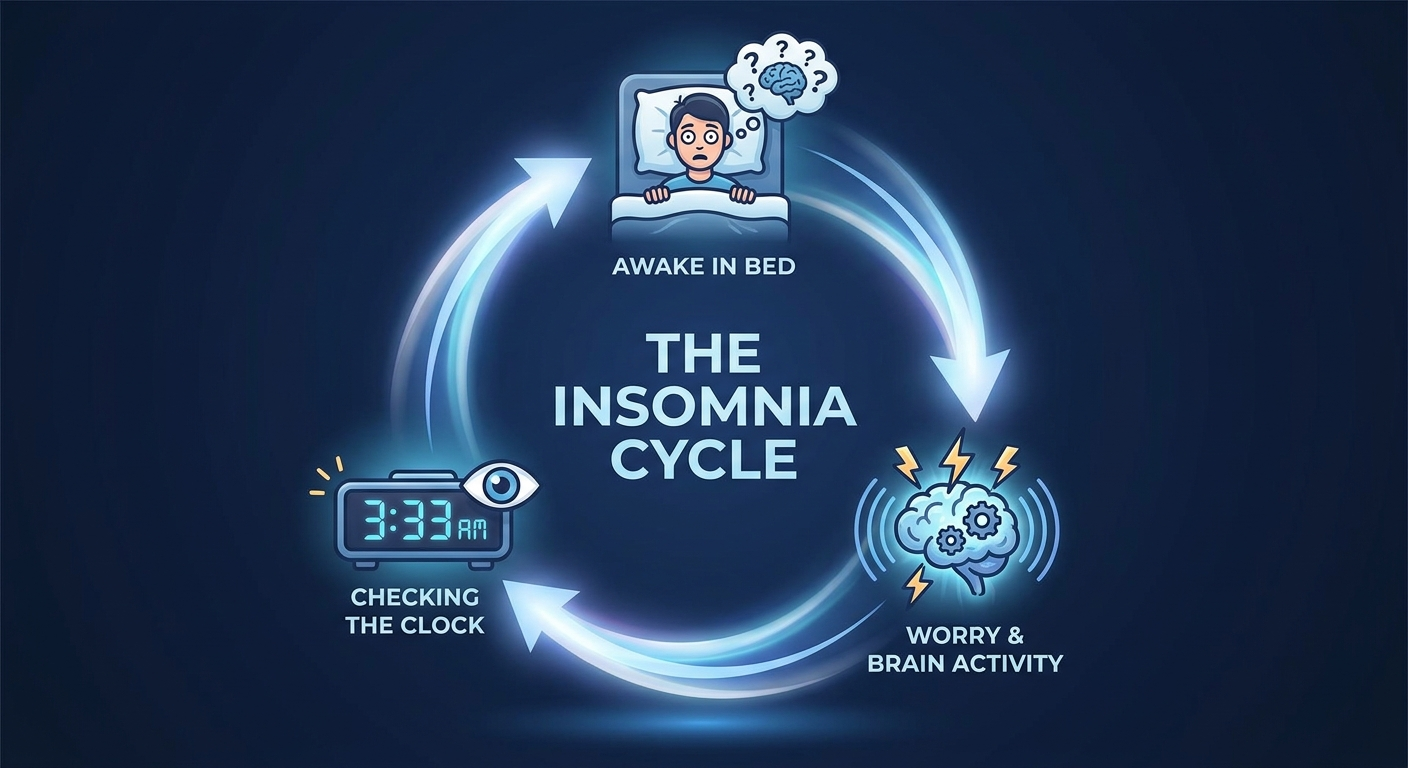
The Insomnia Cycle
A common pattern looks like this: poor sleep → worry about sleep → more alertness and clock-checking → even poorer sleep. Breaking that cycle is a key goal in effective insomnia treatment.
— Addressing schedule, stress, and health contributors together can help unstick the insomnia cycle. —

First Steps to Finding the Right Insomnia Treatment
Start with a simple 1–2 week sleep diary: bedtime and wake time; time to fall asleep and nighttime awakenings; naps; caffeine and alcohol timing; screen time and evening routine. Many people discover they spend far more time in bed awake than realized—insight that directly shapes CBT‑I strategies.
Rule out or address coexisting sleep disorders: insomnia can exist alone or alongside another disorder. Insomnia plus snoring or breathing pauses can point toward sleep-disordered breathing. More on snoring and sleep apnea treatment: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
When to seek professional help (general information): consider support when insomnia occurs most nights, lasts longer than a few months, causes major daytime impairment, or leads to increasing reliance on alcohol or sleep aids. If unsure, see when to see an ENT for sleep-related concerns: https://sleepandsinuscenters.com/blog/when-to-see-an-ent-for-sleep-problems
— A brief diary and a check for underlying conditions can quickly point treatment in the right direction. —

Proven First-Line Treatment: CBT‑I (Cognitive Behavioral Therapy for Insomnia)
CBT‑I is recommended as first-line treatment for chronic insomnia by major professional guidelines and is known for benefits that often last beyond the active treatment period [3][4]. A clinician might say: CBT‑I treats the pattern that keeps insomnia going—so you’re not dependent on perfect circumstances to sleep.
What CBT‑I is (and isn’t): it’s a structured program that targets the behaviors and thoughts that maintain insomnia, not just relaxation or generic advice. Core components include stimulus control (rebuilding the bed as a cue for sleep), sleep restriction or compression (consolidating sleep to reduce time awake in bed), cognitive strategies (reducing catastrophic or rigid sleep thoughts), relaxation training (breathing, muscle relaxation), and supportive sleep hygiene [3][4].
Concrete example of stimulus control: if you’re awake and frustrated, step out of bed for a quiet, dimly lit activity, then return when sleepy—so the bed is associated with sleeping, not struggling.
How long and what to expect: many programs run for several weeks. Progress often looks like less time awake in bed, fewer or shorter awakenings, and more predictable sleep patterns. Confidence and reduced nighttime distress often improve early.
Ways to access CBT‑I: in person, via telehealth, or through digital CBT‑I programs; look for options grounded in established methods. — CBT‑I builds skills that retrain sleep over time, which is why its benefits can outlast the program. —
Medications for Insomnia (When They Help—and Their Limits)
For some, medication can be useful, particularly short-term or as a bridge while CBT‑I skills are built. Guidance emphasizes individualized decisions and recognizes limits in long-term comparative data for many sleep medications [1][4].
Medication may be considered for severe short-term distress, prominent sleep-onset vs sleep-maintenance issues, or a short-term bridge while starting CBT‑I. Many approaches aim for the lowest effective dose for the shortest necessary time, with reassessment due to concerns like tolerance, next-day impairment, falls risk (especially in older adults), and dependence potential [1][4].
— Medications can help as a short-term tool, while CBT‑I addresses the longer-term pattern. —

Newer Option Spotlight: Dual Orexin Receptor Antagonists (DORAs)
Orexin is a wake-promoting signaling system. DORAs block orexin signaling, turning down wake drive to make it easier to fall asleep and stay asleep [1]. FDA-approved DORAs include suvorexant, lemborexant, and daridorexant, with evidence for improved sleep onset and maintenance and generally favorable tolerability [1][2].
In research, DORAs reduce time to fall asleep and improve ability to stay asleep (fewer or shorter awakenings) [1][2]. Some studies suggest small differences among agents, but findings are not definitive and may not apply to every person [1][2]. Potential side effects include next-day sleepiness, unusual dreams, and safety considerations for driving; interactions and other sleep disorders also matter. Decisions are individualized, especially with limited long-term comparative data [1].
Are DORAs a cure? They can be an important tool, but not a universal cure. For durable change—especially in chronic insomnia—CBT‑I remains foundational [3][4].
— DORAs can help turn down wake drive, but CBT‑I remains the cornerstone for durable results. —
Other Evidence-Based Treatment Options (Brief Overview)
Sleep hygiene is a helpful foundation but rarely a standalone cure for chronic insomnia, especially when conditioned arousal is present [4]. Deeper look at sleep hygiene tips: https://sleepandsinuscenters.com/blog/sleep-hygiene-and-its-impact-on-ent-disorders-key-insights
Other prescription options (individualized by symptoms, age, and comorbidities) can include melatonin receptor agonists, low-dose doxepin, and Z‑drugs or benzodiazepines (often with more caution) [4]. Selection focuses on next-day impairment and safety.
Treat the coexisting problem keeping insomnia alive: addressing untreated sleep apnea, reflux, chronic pain, anxiety, or persistent nasal obstruction often improves insomnia more reliably. Nasal breathing and sleep: https://sleepandsinuscenters.com/blog/nasal-breathing-benefits-for-better-sleep-quality
— Pairing insomnia therapy with treatment of contributing conditions usually works better than either approach alone. —
Lifestyle Tips for Better Sleep (Practical, Patient-Friendly)
A better sleep tonight checklist: keep your wake time consistent; set a caffeine cutoff that allows clearance before bedtime; reduce evening alcohol (especially close to bed); use a short, repeatable wind-down with the same steps nightly (dim lights, hygiene routine, light reading, calming music). Consistency beats intensity.

Light, Screens, and Timing
Light powerfully sets the body clock: get morning daylight when possible; dim lights 1–2 hours before bed; reduce stimulating content and bright screens at night. Related reading on blue light: https://sleepandsinuscenters.com/blog/blue-light-and-its-impact-on-ent-related-sleep-disorders-1bca5
Bedroom environment: aim for cool, dark, and quiet; consider consistent background sound if noise is unpredictable. If nighttime nasal breathing is a recurring issue, see: https://sleepandsinuscenters.com/blog/nasal-breathing-benefits-for-better-sleep-quality
What to do when you can’t sleep (CBT‑I style): avoid long stretches awake in bed; if you’re awake too long, get up for a quiet, non-stimulating activity and return when sleepy [4].
— Small, consistent changes to timing, light, and routine can stabilize sleep more than perfect conditions. —
When Insomnia Might Be a Sign of Another Sleep Disorder
Insomnia plus snoring or gasping can suggest sleep-disordered breathing. Overview of snoring and sleep apnea treatment: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
If major daytime sleepiness is present, it raises safety concerns and may point toward another disorder (or insufficient sleep). Identify symptoms to discuss with a clinician: https://sleepandsinuscenters.com/test-your-sleepiness
— If insomnia coexists with snoring, gasping, or marked sleepiness, a targeted sleep evaluation can be helpful. —
FAQs About Curing Insomnia
1) Is there a cure for insomnia? There’s no single cure for everyone, but many experience durable improvement—especially with CBT‑I (first-line) [3][4].
2) How long does CBT‑I take to work? Many programs run several weeks; early gains include less time awake in bed and fewer awakenings, with continued improvements as skills strengthen [3][4].
3) What if I wake at 3 a.m. every night? Early awakenings can relate to stress, circadian timing, alcohol, environment, or coexisting conditions; a sleep diary helps clarify the driver.
4) Are orexin receptor antagonists addictive? DORAs differ from some sedatives, but any sleep medication should be used with clinical oversight and individualized risk/benefit [1][4].
5) Which is better: lemborexant vs daridorexant vs suvorexant? All can improve onset and maintenance; head-to-head and long-term data are limited; small differences may exist but aren’t definitive [1][2].
6) Can I take insomnia medication long-term? Many guidelines emphasize cautious, individualized use and note limited long-term comparative data for many options [1][4].
7) Does melatonin cure insomnia? It can help in some circadian rhythm situations, but it’s not a standalone cure for chronic insomnia [4].
8) Could sleep apnea cause insomnia symptoms? Yes—frequent awakenings and non-restorative sleep can reflect sleep apnea.
9) What’s the best bedtime routine for insomnia? Consistent, calming, and repeatable—paired with a stable wake time and reduced late-night light and screens.
10) When should I see a sleep specialist or ENT? Consider evaluation when insomnia persists for months, significantly affects daytime function, or includes red flags like snoring/gasping or severe sleepiness. Appointments: https://sleepandsinuscenters.com/appointments
Conclusion — A Practical Plan to Move Toward Better Sleep
There’s no one-size-fits-all cure, but there is a proven path: identify contributors, prioritize CBT‑I as first-line, and use medications selectively when appropriate. Newer options like DORAs (suvorexant, lemborexant, daridorexant) are promising for onset and maintenance, but they’re not a universal cure and long-term comparative data remain limited [1][3][4].
If insomnia is persistent or affecting quality of life, a targeted evaluation can clarify what’s driving disruption and guide a plan that fits your symptoms and goals. Book an appointment: https://sleepandsinuscenters.com/appointments
— With the right combination of skills, timing, and targeted care, better sleep is a realistic goal for many people. —
Sources
1. Targeting the Orexin System in the Pharmacological Management of Insomnia (2025) (PMC): https://pmc.ncbi.nlm.nih.gov/articles/PMC12429101/
2. Lemborexant and Daridorexant for the Treatment of Insomnia (2023) (PubMed): https://pubmed.ncbi.nlm.nih.gov/37796657/
3. American College of Physicians (ACP) Guideline (2016): Management of Chronic Insomnia Disorder in Adults: https://www.acpjournals.org/doi/10.7326/M15-2175
4. American Academy of Sleep Medicine (AASM) Practice Standards (2024): https://aasm.org/clinical-resources/practice-standards/
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.