CBT Insomnia Training: Evidence-Based CBT-I Techniques to Improve Sleep
If you’ve tried “all the sleep tips” and you’re still lying awake, it may be time for a more structured approach. CBT insomnia training is a practical, skills-based way to retrain sleep—not just “optimize” it. It’s based on cognitive behavioral therapy for insomnia (CBT-I), an evidence-based program designed to break the insomnia cycle and rebuild consistent, restorative sleep over time. Overview and mechanisms: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
Think of CBT-I like physical therapy for sleep: you don’t “willpower” your way into better movement—you follow a plan, practice the right drills, and track progress.
Why “CBT Insomnia Training” Is Different From Generic Sleep Tips
The problem with “sleep hygiene only”
Sleep hygiene (like keeping the bedroom cool or cutting caffeine late in the day) can help—but it often isn’t enough for chronic insomnia. When insomnia is persistent, the issue is frequently not a lack of tips.
More often, it’s a learned pattern: the bed becomes associated with wakefulness, worry shows up on cue, and “coping” behaviors accidentally keep insomnia going (sleeping in, going to bed early “just in case,” or spending long stretches in bed awake).
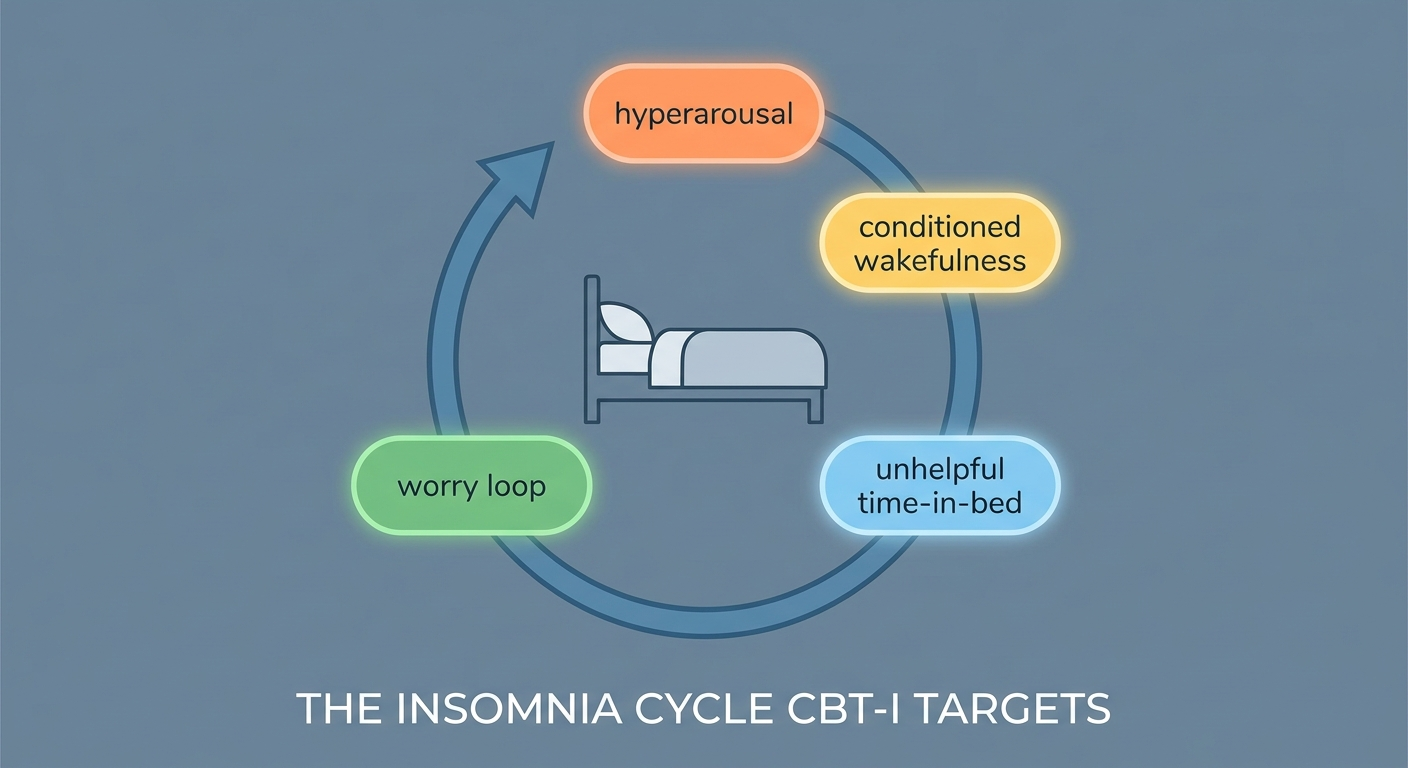
What CBT-I targets (the insomnia cycle)
- Hyperarousal (your body and brain staying “on” at night)
- Conditioned wakefulness (bed = stress/alertness instead of sleep)
- Unhelpful sleep behaviors (extra time in bed, irregular sleep windows)
- Worry loops (“What if I don’t sleep?” → more arousal → less sleep)
This is one reason CBT-I is delivered as a structured, multi-component program—not a single trick. Mechanisms overview: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
CBT-I is first-line treatment for chronic insomnia
Major clinical guidelines recognize CBT-I as a first-line approach for ongoing insomnia, rather than relying only on sleep medications. First-line discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
— Italic summary: CBT insomnia training targets the patterns that keep insomnia going and applies a structured plan to reverse them. —
Quick Refresher—What Counts as Insomnia?
Common insomnia symptoms (sleep initiation and maintenance)
- Trouble falling asleep
- Waking up frequently or too early
- Non-restorative sleep plus daytime impact (fatigue, concentration problems, irritability)
A common “real life” presentation: you’re exhausted all day, but the moment you get into bed your brain starts problem-solving.
When insomnia becomes “chronic”
A standard clinical shorthand: at least 3 nights per week for 3 months or longer, with meaningful daytime impairment.
Red flags that should prompt medical evaluation (not just CBT-I)
- Loud snoring, gasping/choking, or witnessed breathing pauses (possible obstructive sleep apnea/sleep-disordered breathing)
- Restless legs syndrome symptoms (urge to move legs, worse at night)
- New or worsening depression/anxiety, suicidal thoughts
- Significant daytime sleepiness with safety concerns (driving/work)
If any of these apply, medical evaluation is recommended. See: When to see a specialist for sleep issues https://sleepandsinuscenters.com/blog/when-to-see-an-ent-for-sleep-problems
— Italic summary: If red-flag symptoms are present, prioritize a medical evaluation before or alongside CBT-I. —
Causes of Insomnia (Patient-Friendly Breakdown)
“Predisposing, precipitating, perpetuating” model (simple explanation)
- Predisposing: baseline vulnerability (light sleep, stress sensitivity, family history)
- Precipitating: a trigger (illness, work stress, travel, grief)
- Perpetuating: patterns that keep insomnia going even after the trigger fades
CBT-I primarily targets the perpetuating factors—because those are the pieces you can change through training and structure.
Common perpetuating causes CBT-I is designed to address
- Spending too much time in bed “trying” to sleep
- Napping as a survival strategy (which can reduce sleep drive at night)
- Clock-watching and sleep tracking anxiety
- Caffeine/alcohol timing and inconsistent schedules
Insomnia with other conditions (comorbid insomnia)
Insomnia often overlaps with anxiety, depression, chronic pain, medical illness, and sleep-disordered breathing. CBT-I can still be useful in these contexts and is widely studied in comorbid insomnia. Applications/comorbidities: https://pmc.ncbi.nlm.nih.gov/articles/PMC9319701/
— Italic summary: Understanding what’s keeping insomnia going makes it easier to target with the right CBT-I skills. —
What CBT-I Includes (The Core Components)
Sleep diary and baseline measurements (your “training data”)
A sleep diary is the foundation of CBT-I. It typically tracks:
- Bedtime, lights out, estimated time to fall asleep
- Night awakenings and wake time
- Naps
- Caffeine/alcohol timing
- Any medications or late-evening nicotine use
Many programs also use the Insomnia Severity Index (ISI) as a progress metric—useful for seeing whether symptoms improve week to week.
The core CBT-I components
- Stimulus control (rebuilds bed = sleep association)
- Sleep Restriction Therapy (SRT) or sleep compression (consolidates sleep to improve efficiency)
- Cognitive therapy (modifies thoughts that fuel hyperarousal)
- Relaxation and wind-down strategies (arousal reduction)
- Sleep education and circadian basics
- Targeted sleep hygiene (supportive, not standalone)
Common mistakes that slow progress
- Guessing without logging a sleep diary
- Staying in bed awake for long stretches
- Changing the schedule too often or too quickly
- Turning relaxation into a “performance” task
— Italic summary: Track first, then apply stimulus control and a data-guided schedule while adding cognitive and wind-down tools. —
Technique 1 — Stimulus Control (Rebuilding the Bed = Sleep Association)
Who benefits most
This is especially helpful when you feel alert the moment you get into bed, or you associate bedtime with dread, planning, or problem-solving. The goal: teach your brain that bed predicts sleep—not stress.
The stimulus control “rules” (simple and specific)
- Use the bed for sleep and intimacy only.
- If you’re awake around 15–20 minutes, get out of bed (use your best guess—avoid clock-watching).
- Keep wake time consistent.
- Avoid naps (or limit/strategize them only if a clinician-built plan includes them).
Troubleshooting common barriers
- Concern about waking a partner: plan a quiet “reset” spot (dim light, low stimulation).
- Too tired to get up: try a brief, minimum-effective reset (sit elsewhere for a few minutes) rather than staying in bed frustrated.
— Italic summary: Leave the bed when awake so the bed reliably predicts sleep again. —

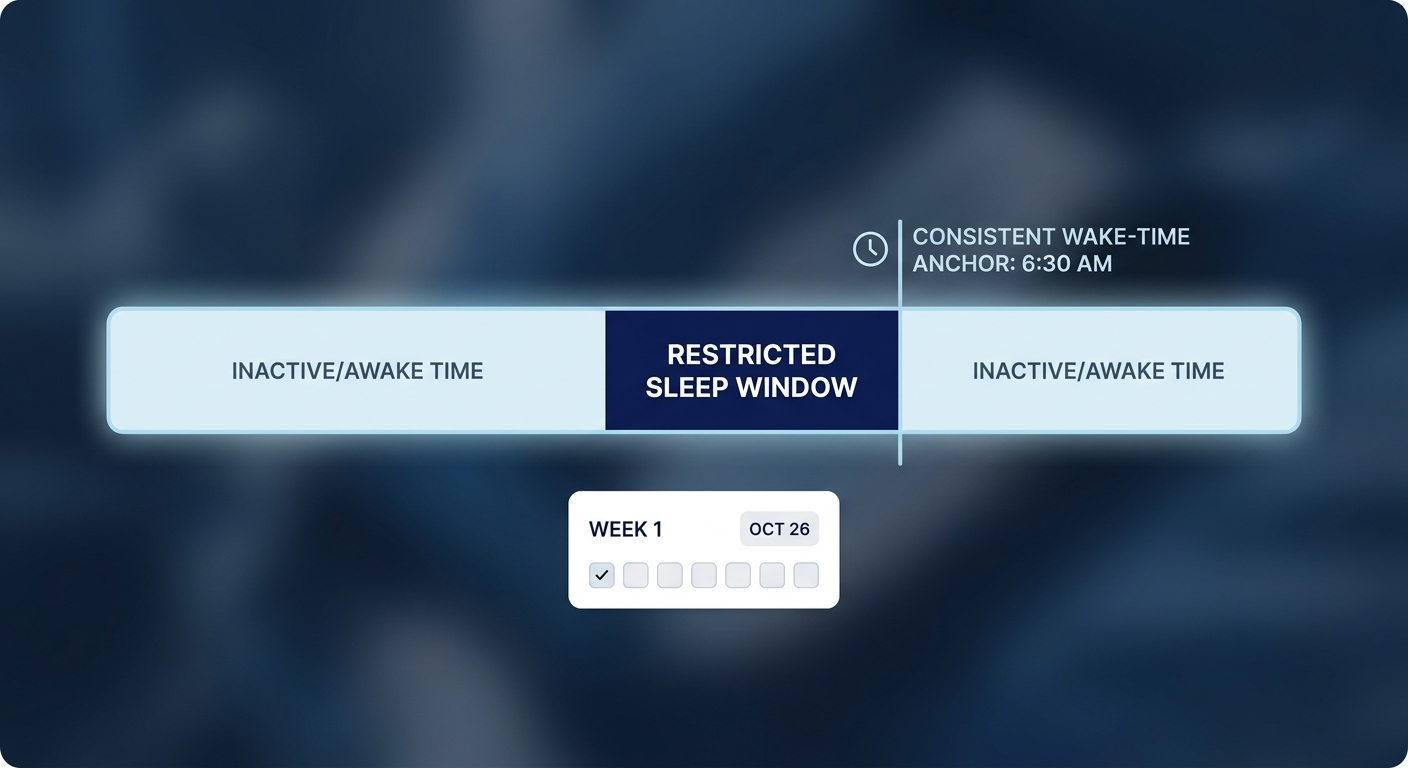
Technique 2 — Sleep Restriction Therapy (SRT) or Sleep Compression: A Common and Effective Way to Improve Sleep Efficiency
What it is (and what it is not)
SRT is not “pushing through exhaustion” as a lifestyle. It’s a short-term, structured schedule that reduces time in bed to better match actual sleep—so sleep becomes deeper, more consolidated, and less fragmented.
Step-by-step setup (education-only overview)
- Gather 1–2 weeks of sleep diary data to estimate average total sleep time.
- Choose a consistent wake time (the anchor).
- Set a time-in-bed window close to actual sleep time (programs often include a minimum safety floor).
- Adjust weekly based on sleep efficiency trends.
What to expect in the first couple of weeks
Some people notice temporary sleepiness early on, then:
- Faster sleep onset
- Fewer/shorter awakenings
- More stable sleep as weeks progress
Safety notes
Because SRT can increase sleepiness at first, it may not be ideal to start during high-risk weeks (for example, heavy driving or safety-sensitive work). People with certain medical or psychiatric conditions may need closer supervision. Educational overview: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
— Italic summary: Short-term, data-guided limits on time in bed can help your sleep become deeper and more reliable. —
Technique 3 — Cognitive Restructuring (Changing the Thoughts That Keep You Awake)
Common insomnia thoughts CBT-I targets
- “If I don’t get 8 hours, tomorrow is ruined.”
- “I’ll never sleep normally again.”
These thoughts are understandable—especially after weeks or months of poor sleep—but they can spike arousal exactly when your body needs to settle.
A simple 3-step thought tool
- Identify the thought.
- Rate belief (0–100%) and name the feeling (anxious, frustrated, helpless).
- Generate a more balanced thought, then re-rate belief.
The goal isn’t forced positivity—it’s a more realistic inner script that doesn’t trigger a stress response.
Reducing “sleep effort”
Many people sleep better when they shift from “trying to sleep” to “allowing sleep.” In CBT insomnia training, that often means focusing on the process (consistent wake time, sleep window, stimulus control) and letting sleep be the outcome—not the nightly test.
— Italic summary: A calmer, more balanced inner script reduces arousal and makes space for sleep to emerge. —

Technique 4 — Relaxation and Wind-Down Strategies (Arousal Reduction)
Breathing techniques
Gentle, steady breathing (often with a slightly longer exhale than inhale) can signal safety to the body. The aim is settling, not “knocking yourself out.”
Progressive muscle relaxation (PMR)
Tense and release muscle groups to reduce physical tension you may not notice until you intentionally let it go.
Guided imagery or body scan
These practices help redirect attention away from sleep-monitoring (“Am I asleep yet?”) and toward neutral sensations or calming scenes.
When relaxation helps most—and when it backfires
Relaxation helps when it’s treated as practice, not performance. If it becomes another “I must do this perfectly to sleep” task, return to stimulus control principles.
— Italic summary: Use wind-down practices to lower arousal, but don’t turn them into a test. —

Technique 5 — Circadian and Lifestyle Supports (The “Amplifiers” of CBT-I)
Morning light and a consistent wake time (circadian anchor)
Morning light and a steady wake time help stabilize the circadian rhythm that supports nighttime sleepiness. Even after a rough night, protecting the wake-time anchor is often key.
Caffeine, nicotine, and alcohol timing
Timing matters. Many CBT-I plans review how afternoon caffeine, evening nicotine, or alcohol near bedtime affects awakenings and lighter sleep.
Exercise timing
Regular activity supports sleep for many people. Some prefer earlier exercise; others do fine later. Tracking it in your sleep diary can reveal your personal pattern.
Bedroom environment checklist
- Cooler room temperature
- Darkness
- Minimizing disruptive noise (or using steady background sound)
Screens and blue light (realistic approach)
Instead of “no screens ever,” many people do better with a realistic wind-down: dimmer screens, calmer content, and a clear “end point” before trying to sleep.
— Italic summary: Small, consistent circadian and lifestyle supports make CBT-I work easier and more durable. —
A Sample 6–8 Week CBT Insomnia Training Plan (What a Program Looks Like)
Week 0–1: Assessment, sleep diary, goal setting
Track your baseline and identify patterns. Consider adding the ISI for a measurable starting point.
Week 2: Stimulus control
Apply stimulus control therapy consistently and troubleshoot obstacles (partner sleep, small kids, limited space).
Week 3–4: SRT or sleep compression with weekly adjustments
Begin SRT or sleep compression and adjust gradually based on diary data.
Week 4–6: Cognitive tools and worry management
Add cognitive restructuring and set a plan for “worry time” earlier in the day so it doesn’t move into bed.
Week 6–8: Relapse prevention and “what to do after a bad night”
Build a personal flare-up plan (for example: protect wake time, avoid spending extra hours in bed, return to stimulus control).
— Italic summary: CBT-I is typically a 6–8 week training process with measurement, structured practice, and weekly fine-tuning. —
Digital CBT-I (dCBT-I): Evidence, Options, and How to Choose
Can digital CBT-I work? What the research suggests
Research reviews and trials suggest digital CBT-I can improve insomnia severity and sleep quality for many people, and may also improve mood symptoms for some people. Evidence overview: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/ Comorbidities discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC9319701/
Evidence in older adults
A 2025 randomized trial supports benefits of digital CBT-I approaches in older adults, an important group for access and scalability. Nature 2025 RCT: https://www.nature.com/articles/s41746-025-01847-0
Example digital program trial: Headspace Sleep Program
A 2025 randomized trial reported improvements in sleep outcomes in a digital sleep program format. JMIR mHealth 2025 RCT: http://mhealth.jmir.org/2025/1/e68665
Popular digital CBT-I formats
- Self-guided programs: accessible and often lower cost, though adherence can be harder without support.
- Guided programs (coach/therapist support): better accountability and troubleshooting, but may cost more or be less available.
Examples patients may see online (not endorsements—just examples to evaluate):
- Restful (CBT-I diary/app listing): http://apps.apple.com/us/app/restful-cbt-i-insomnia-diary/id1611283700
- Somnio (company presence): http://linkedin.com/company/somnio
How to choose a dCBT-I safely
Look for: sleep diary tracking, stimulus control, SRT or sleep compression, cognitive tools, schedule adjustments based on data, and clear guidance on when to seek evaluation.
— Italic summary: Digital CBT-I can extend access; look for programs that include diary-driven scheduling plus stimulus control and cognitive tools. —
Clinician and Coach Training (Why “Fidelity” Matters)
What “CBT-I fidelity” means
CBT-I works best when delivered as intended: diary → schedule → adjustments → cognitive/relaxation skills. That structure is part of why CBT insomnia training is different from generic advice. Structured multi-component treatment: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
Questions patients can ask
- Have you been trained specifically in CBT-I?
- Do you use sleep diaries and formal scheduling?
- How do you adjust the plan based on weekly data?
Emerging training pathways
Training pathways are expanding through standardized curricula, multi-session programs, and supervision models.
— Italic summary: Provider training and fidelity to the CBT-I model meaningfully influence outcomes. —
When CBT-I Isn’t Enough (Or When to Combine Approaches)
If sleep apnea is present, both conditions may need to be addressed as part of care
Snoring and breathing pauses can mimic or worsen insomnia. Treating a breathing-related sleep disorder can make CBT-I more effective and sustainable. Learn more about evaluation and options: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
Medications: where they may fit
Some people use medication short term while building CBT-I skills. Any changes to prescriptions should be handled with your clinician.
Mental health support when needed
If insomnia is closely tied to panic, trauma, severe depression, or substance use, additional mental health support can be an important part of care.
— Italic summary: Address other sleep or mental health conditions alongside CBT-I to improve long-term results. —
FAQs About CBT Insomnia Training / CBT-I
How long does CBT-I take to work?
Many people notice early changes within a few weeks, with more stable improvement across a 6–8 week program—especially when diaries and weekly adjustments are used.
Will SRT make me more tired at first?
It can. That short-term sleepiness is one reason programs emphasize safety planning and avoiding high-risk situations during early adjustments.
Is CBT-I safe for older adults?
Research suggests digital CBT-I approaches can benefit older adults. Nature 2025 RCT: https://www.nature.com/articles/s41746-025-01847-0
Can CBT-I help anxiety or depression symptoms too?
Studies discuss improvements in insomnia with potential secondary benefits for mood symptoms in some populations. Comorbidities/applications: https://pmc.ncbi.nlm.nih.gov/articles/PMC9319701/
What if I wake up at 3 a.m. every night?
This common pattern often responds to a combination of stimulus control, a consistent wake time, and schedule adjustments informed by a sleep diary.
Should I track sleep with a wearable?
Wearables can be useful for trends, but they can also increase sleep-related anxiety for some people. Many CBT-I programs prioritize the sleep diary as the main “training data.”
Can I do CBT-I if I have chronic sinus congestion or breathing issues at night?
CBT-I skills can still help, but breathing issues may interfere with sleep quality and continuity. If you have congestion plus snoring or mouth breathing, consider evaluation by a qualified sleep specialist or ENT to rule out contributing factors. Related resource: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
— Italic summary: Personalize CBT-I with data, stay consistent, and seek evaluation for red flags or coexisting conditions. —
Key Takeaways (Short Summary)
- CBT-I is an evidence-based first-line approach for chronic insomnia. Evidence overview: https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
- The “big movers” are stimulus control, SRT or sleep compression, and cognitive tools.
- Digital CBT-I can expand access when trained clinicians are limited. Older adults RCT: https://www.nature.com/articles/s41746-025-01847-0 Headspace Sleep Program RCT: http://mhealth.jmir.org/2025/1/e68665
— Italic summary: A structured CBT-I plan—plus consistent follow-through—can meaningfully improve sleep for many people. —
Call to Action (Patient-Friendly)
If your insomnia is persistent—or you suspect sleep-disordered breathing—get the right evaluation
If sleep problems are affecting your days, it helps to get clarity on what’s driving them (and whether insomnia overlaps with breathing-related sleep issues).
Next steps (Sleep and Sinus Centers of Georgia):
- Check your daytime sleepiness: https://sleepandsinuscenters.com/test-your-sleepiness
- When to see a specialist for sleep issues: https://sleepandsinuscenters.com/blog/when-to-see-an-ent-for-sleep-problems
- Rule out sleep apnea (a common insomnia mimic): https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
- Book an appointment: https://www.sleepandsinuscenters.com/
Medical disclaimer: This article is for general education and is not a substitute for medical advice, diagnosis, or treatment. If you have safety concerns (e.g., severe daytime sleepiness, suicidal thoughts, or symptoms of sleep apnea), seek prompt evaluation from a qualified clinician.
Citations (reference list)
1. CBT-I overview / multi-component treatment (PMC): https://pmc.ncbi.nlm.nih.gov/articles/PMC10002474/
2. CBT-I applications and comorbidities (PMC): https://pmc.ncbi.nlm.nih.gov/articles/PMC9319701/
3. Digital CBT-I RCT in older adults (Nature, 2025): https://www.nature.com/articles/s41746-025-01847-0
4. Headspace Sleep Program RCT (JMIR mHealth, 2025): http://mhealth.jmir.org/2025/1/e68665
5. Restful CBT-I app listing (commercial): http://apps.apple.com/us/app/restful-cbt-i-insomnia-diary/id1611283700
6. Somnio company page (commercial): http://linkedin.com/company/somnio
“This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.”
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.