Cannabis Use and Its Impact on Sleep Apnea and ENT Health
Cannabis is increasingly discussed as a “sleep aid,” so it’s understandable that people also wonder about cannabis use and sleep apnea. The challenge is that obstructive sleep apnea (OSA) isn’t primarily a problem of falling asleep—it’s a problem of airflow and breathing stability during sleep.
At the same time, inhaled cannabis can affect the nose, throat, and mouth in ways that matter to both sleep and daytime quality of life—especially if congestion, dry mouth, hoarseness, or recurrent sinus symptoms are already part of your picture.
Below is a patient-friendly overview of what research suggests, what remains uncertain, and why ENT (ear, nose, and throat) health is a key part of the conversation.
Bottom line up front: OSA is an airway problem, and inhaled cannabis can irritate that airway.
Quick Take: Is Cannabis a Safe or Effective Sleep Apnea Treatment?
The headline answer: Small, short-term studies suggest synthetic cannabinoids such as dronabinol may modestly improve some sleep apnea measures in certain people, but evidence remains limited. Side effects (including daytime sleepiness) are common, follow-up is short, and real-world safety is uncertain. Because of these gaps, major sleep organizations do not recommend medical cannabis as a treatment for OSA. (AASM, 2018)
In short, current evidence does not support cannabis as a reliable or recommended treatment for OSA.
The biggest ENT concern: When it comes to cannabis and ENT health, inhalation—especially smoking—raises the most consistent concerns. Research and clinical literature link inhaled cannabis with sinus and nasal irritation, throat/voice changes, and oral health issues. Newer observational data also report an association between cannabis-use disorder and increased head-and-neck cancer risk, though causation has not been established and confounding factors (like tobacco and alcohol) are difficult to fully separate. (Phulka et al., 2021; Rosen et al., 2019; Gallagher et al., 2024; ADA, 2023)
If you already struggle with congestion, hoarseness, or dry mouth, inhaled cannabis can make those issues worse.
What we know / what we don’t know (simple summary):
- We know: Small studies of dronabinol for obstructive sleep apnea have shown modest improvements in some measures; inhaled cannabis is frequently linked to ENT and oral irritation.
- We don’t know (yet): Whether cannabinoid approaches meaningfully improve long-term OSA outcomes (like cardiovascular risk) or are safe/effective for long-term use in typical real-world patients.

Sleep Apnea Basics (So the Cannabis Question Makes Sense)
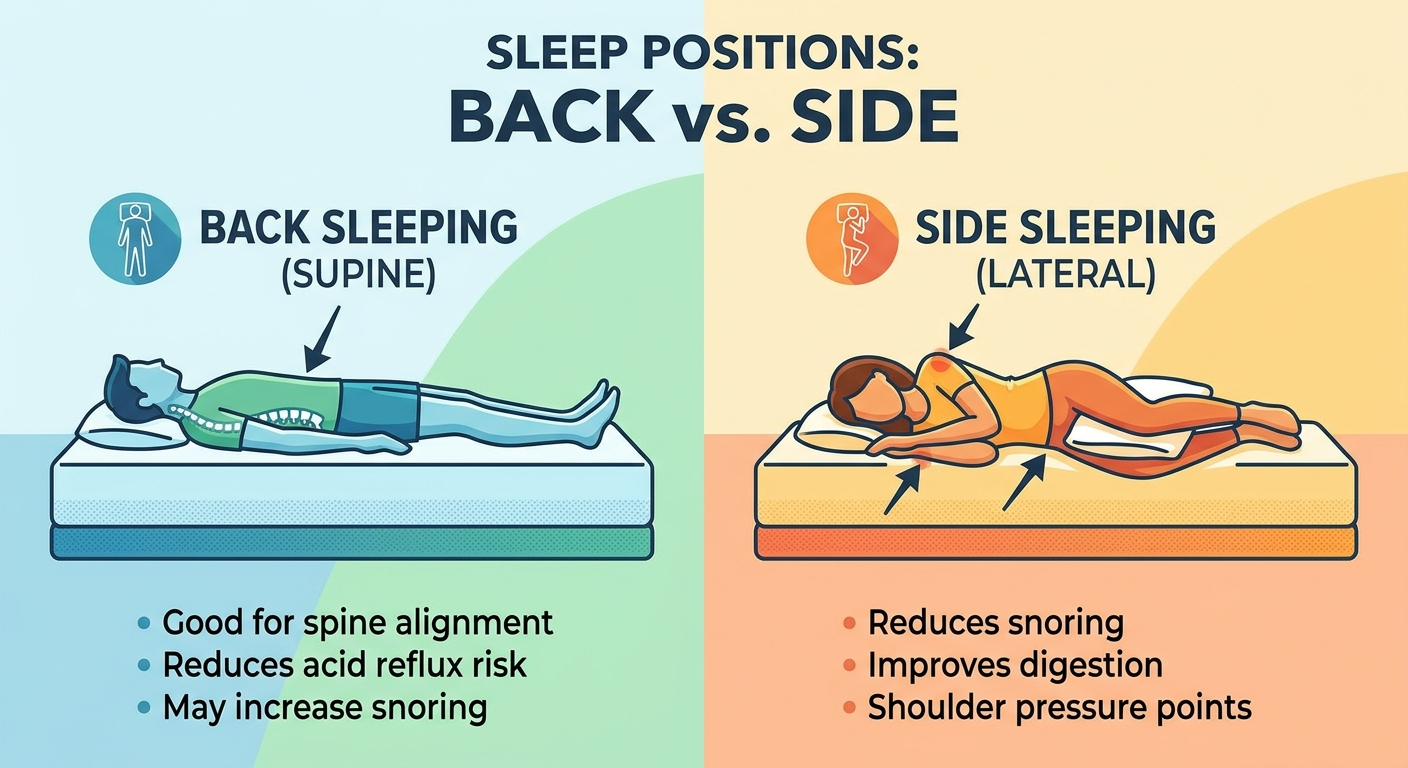
What obstructive sleep apnea (OSA) is: OSA is repeated collapse or narrowing of the upper airway during sleep. These events can reduce oxygen levels and fragment sleep—even if someone doesn’t fully wake up. Think of OSA less like “insomnia” and more like a bendy straw—when surrounding muscles relax during sleep, the straw intermittently kinks.
OSA is an airway stability problem, not a falling-asleep problem.
Common symptoms patients notice:
- Loud snoring
- Witnessed pauses in breathing
- Gasping or choking at night
- Morning headaches
- Dry mouth
- Insomnia or restless sleep
- Daytime sleepiness or fatigue
- Concentration problems/“brain fog”
A common comment clinicians hear: “I sleep all night, but I never feel rested.” That “slept through it” feeling can still happen in OSA because the brain may not fully wake up—even though breathing is repeatedly disrupted.
Why treating OSA matters: Untreated OSA is associated with cardiovascular risk, mood and cognitive effects, safety concerns (including drowsy driving), and reduced quality of life.
Treating OSA helps protect heart health, daytime functioning, and quality of life.
Standard, evidence-based treatments: Effective care often combines multiple strategies, such as CPAP/APAP, oral appliance therapy, weight management, positional therapy, addressing nasal obstruction/allergies, and select surgeries when appropriate. For an overview, see Sleep and Sinus Centers of Georgia’s page on sleep apnea treatment options: https://sleepandsinuscenters.com/snoring-sleep-apnea-treatment
Relaxation at bedtime is not the same as fixing airway collapse.
Why People Consider Cannabis for Sleep (and Where Confusion Starts)
Cannabis may “feel” like it helps sleep: Some people report easier sleep onset or reduced nighttime anxiety. Sedation can be interpreted as “better sleep,” especially in the short term. For example, someone might take an edible and fall asleep faster, then assume their “sleep problem” is solved—even if they still snore loudly or wake with a headache.
“Sleep improvement” is not the same as treating OSA: OSA is a breathing/airway disorder. Feeling sleepier or falling asleep faster doesn’t necessarily mean breathing events improved. Increased sedation could potentially make it easier to sleep through breathing disruptions—without reducing them.
THC vs CBD vs synthetic cannabinoids (plain-language definitions):
- THC: The intoxicating component; can cause sedation and next-day impairment in some people.
- CBD: Non-intoxicating; its effects on sleep and OSA specifically are not well-established.
- Synthetic cannabinoids (e.g., dronabinol): Prescription, pharmaceutical-grade compounds studied under standardized dosing—different from dispensary products.
Sedation is not a substitute for treating airway obstruction.

What Research Says About Cannabinoids for OSA (Dronabinol and Small Trials)
What studies have shown (in simple terms): Small studies of dronabinol for obstructive sleep apnea have shown modest improvements in AHI (apnea–hypopnea index) for some participants and improvements in subjective daytime sleepiness in some groups. These findings are generally described as “promising but preliminary,” not definitive. (AASM, 2018 and reviews)
Why the evidence is still considered limited:
- Small sample sizes
- Short study duration (limited long-term insight)
- Varying doses and mixed results
- Unclear impact on outcomes beyond AHI (like blood pressure, cardiovascular risk, sustained symptom control)
Side effects and safety flags: Commonly reported concerns include somnolence (sleepiness). Broader cautions include potential cognitive effects, driving safety risks, interactions with other sedating substances, and dependence risk in vulnerable individuals.
What major sleep societies recommend: The American Academy of Sleep Medicine (AASM) does not support cannabis as a treatment for OSA due to insufficient evidence and safety concerns. (AASM, 2018)
Promising signals remain preliminary, with limited, short-term data and notable side effects; cannabis is not a replacement for proven OSA therapy.
Why Clinicians Are Especially Cautious About Smoked Cannabis in Sleep Apnea
Sedation can mask symptoms without fixing breathing: If someone feels less aware of awakenings or discomfort, they may perceive improvement—while apneas still occur.
Upper-airway irritation and inflammation can work against breathing: Smoke, heat, and particulate exposure may irritate nasal and throat tissues. For people prone to congestion, swelling, or inflammation, this can be counterproductive to airflow.
Safety concerns if you already have untreated OSA: Both untreated OSA and sedating substances can contribute to next-day impairment. This is one reason organizational guidance emphasizes safety when considering cannabis use and sleep apnea. (AASM, 2018)
If you have OSA, added sedation and airway irritation can work against safer, clearer breathing.

ENT & Oral Health: What Inhaled Cannabis Can Do to the Nose, Throat, and Mouth
Nose & sinuses (congestion, rhinitis, sinusitis): The ENT literature includes reported associations between inhaled cannabis and chronic rhinosinusitis/sinusitis and rhinitis-like symptoms and congestion. Evidence quality varies and findings are heterogeneous, but irritation and inflammation are recurring themes. (Phulka et al., 2021) Learn more about sinus inflammation at: https://sleepandsinuscenters.com/chronic-sinusitis
Throat & voice (hoarseness, laryngeal irritation): A systematic review found associations between cannabis inhalation and hoarseness/voice changes and inflammatory or irritative changes affecting the vocal folds. (Rosen et al., 2019)
Mouth, teeth, and gums (dry mouth, periodontal disease, lesions): Cannabis has been associated with oral health issues such as xerostomia (dry mouth), periodontal disease, and leukoplakia and other mucosal changes/lesions. (ADA, 2023)
A concrete example: if cannabis worsens dry mouth overnight, you may wake up with a “cotton mouth” feeling—then compensate with mouth breathing because the nose feels irritated or congested, which can further dry the throat and worsen morning discomfort.
Head-and-neck cancer signals: A large observational study reported an association between cannabis-use disorder and increased head-and-neck cancer risk, though causation has not been established. Confounding factors (tobacco, alcohol, HPV) remain important. (Gallagher et al., 2024)
For many patients, how cannabis is used matters as much as whether it is used at all—especially for the nose, throat, and mouth.
Mode of Use Matters (Smoking vs Vaping vs Edibles vs Pharmaceuticals)
Smoking (highest local ENT exposure): Smoking tends to have the most direct exposure to nasal, throat, and oral tissues—and the most consistent links in the literature to irritation and lesions. (Phulka et al., 2021; ADA, 2023; Rosen et al., 2019)
Vaping: Vaping may reduce some combustion byproducts, but it still exposes ENT tissues to heated aerosols and potential irritants. For a deeper look: https://sleepandsinuscenters.com/blog/vaping-effects-on-ent-health-understanding-risks-and-impact
Edibles/tinctures: These avoid direct smoke exposure to ENT tissues, but systemic effects (sleepiness, interactions, delayed onset, variable dosing) may still occur.
Pharmaceutical cannabinoids (like dronabinol): Pharmaceutical products differ from dispensary cannabis in purity and dosing control, but they are still not endorsed for OSA due to limited evidence and safety concerns. (AASM, 2018)
Avoiding inhalation reduces local ENT exposure but does not eliminate systemic risks—or prove effectiveness for OSA.
If You Have Sleep Apnea and Use Cannabis: Practical, Patient-Friendly Tips (Educational)
- Don’t replace proven OSA therapy with cannabis without discussing it with a sleep professional.
- Route matters for ENT irritation: inhalation typically creates more direct nose/throat/mouth exposure than non-inhaled routes.
- Be cautious with other sedating substances (like alcohol or sleep medications) because combined impairment risk can increase.
- Track changes over time: worsening snoring, morning headaches, increased daytime sleepiness, recurrent sinus infections, or persistent hoarseness can be useful signals to report.
- Share specifics (how often, which route—smoke/vape/edible—and whether tobacco is also used). This helps clinicians interpret symptoms accurately.
Work with your clinician, and do not substitute cannabis for proven therapies.
Treatments That Help Both OSA and ENT Health (Evidence-Based Options)
- Evaluate nasal breathing issues (allergic rhinitis, chronic sinusitis, deviated septum, turbinate enlargement)
- Manage inflammation triggers (saline rinses, allergy-directed strategies, clinician-directed nasal treatments when appropriate)
- Lifestyle approaches with strong OSA benefit (weight management, positional therapy, consistent sleep schedule, reflux management when present)
- Improve CPAP tolerance (mask refitting, humidification adjustments, and addressing nasal blockage)
Addressing the entire airway often improves both sleep quality and daytime comfort.
When to See an ENT or Sleep Specialist (Red Flags)
Sleep-related red flags:
- Witnessed apneas, gasping, or choking
- Severe daytime sleepiness
- Drowsy driving
- Resistant high blood pressure
ENT/oral red flags (especially if you smoke/vape cannabis):
- Hoarseness lasting more than 2–3 weeks
- Mouth sores or persistent white patches
- Persistent one-sided nasal obstruction or recurrent nosebleeds
- Neck mass, trouble swallowing, or unexplained weight loss
Early evaluation can prevent complications and speed safer, more effective care.
FAQs (SEO-Friendly)
Can marijuana cure sleep apnea? Current evidence does not support marijuana as a cure. The AASM does not recommend cannabis for treating OSA due to limited evidence and safety concerns. (AASM, 2018)
Is CBD safer than THC for sleep apnea? Data on CBD for OSA specifically are limited. “Safer” depends on dose, other medications/substances, medical history, and side effects—so it’s best treated as an individualized risk discussion.
What’s the difference between cannabis and dronabinol in the studies? Dronabinol is pharmaceutical-grade with standardized dosing. Dispensary products vary widely in THC/CBD content and delivery, so study results on dronabinol do not automatically apply to typical cannabis use.
Has smoking cannabis been associated with sinus infections or sinus symptoms? Studies and reviews report associations between inhaled cannabis and sinusitis/rhinitis symptoms, though confounding factors exist. Irritation and inflammation are consistent concerns in the ENT literature. (Phulka et al., 2021)
Can cannabis cause hoarseness or voice damage? Cannabis inhalation has been associated with voice changes and vocal fold irritation in voice-focused research. (Rosen et al., 2019)
Does cannabis increase head and neck cancer risk? Older research has been mixed, but a newer large observational study found an association between cannabis-use disorder and increased head-and-neck cancer risk. This does not prove causation, and confounding factors remain important. (Gallagher et al., 2024)
Key Takeaways (1-minute recap)
What’s supported: Dronabinol shows modest improvements in small trials, but evidence remains limited.
What’s not recommended: Medical cannabis is not recommended for OSA by the AASM. (AASM, 2018)
What to avoid (from an ENT perspective): Smoked cannabis has the strongest association with ENT and oral irritation, which matters for airway comfort and symptoms.
What to do next: If symptoms suggest OSA or persistent ENT/oral issues are present, an evaluation and evidence-based treatment plan can be more reliable than unproven approaches—especially when navigating cannabis use and sleep apnea.
When in doubt, lean on proven therapies and expert evaluation.
CTA: Ready for a clearer plan?
If you’re dealing with snoring, suspected sleep apnea, chronic congestion, or lingering throat/voice symptoms, you can book an appointment with the team at Sleep and Sinus Centers of Georgia here: https://www.sleepandsinuscenters.com/
References
1. American Academy of Sleep Medicine (AASM). Position statement: medical cannabis and OSA (2018). https://pmc.ncbi.nlm.nih.gov/articles/PMC5886446/
2. Phulka JS et al. Scoping review: cannabis and otolaryngology effects (2021). https://pmc.ncbi.nlm.nih.gov/articles/PMC8474823/
3. Rosen CA et al. Systematic review: cannabis and voice/vocal fold findings (2019). https://pubmed.ncbi.nlm.nih.gov/31393535/
4. Gallagher TJ et al. Cohort study: cannabis-use disorder and head-and-neck cancer risk (2024). https://jamanetwork.com/journals/jamaotolaryngology/articlepdf/2822269/jamaotolaryngology_gallagher_2024_oi_240052_1740605205.56535.pdf
5. American Dental Association (ADA). Cannabis: oral health effects (2023). https://www.ada.org/resources/ada-library/oral-health-topics/cannabis-oral-health-effects
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.