Are You Unconscious When You Sleep? Sleep Consciousness Explained
Many people ask, “are you unconscious when you sleep?” It’s a fair question—sleep can feel like a total “shutdown,” especially when you’re hard to wake, sleep through an alarm, or feel confused after being awakened.
What science shows is more nuanced: sleep is a distinct brain state with changing levels of awareness, not a blank, unconscious void. The brain cycles through sleep stages and remains selectively responsive to some stimuli, which is why you can still wake up when it matters (NCBI Bookshelf; Cleveland Clinic; TeachMePhysiology).
Quick Answer: Sleep Is “Altered Consciousness,” Not Total Unconsciousness
In everyday language, “unconscious” often means “not aware of anything.” In medicine, unconsciousness usually implies an abnormal state where a person can’t be awakened or doesn’t respond appropriately (for example, coma).
Sleep is different. During normal sleep, awareness and responsiveness decrease—especially in deep sleep—but the sleeping brain can still process some information and awaken depending on arousal threshold. This is why sleep is not the same as coma or anesthesia (NCBI Bookshelf; Cleveland Clinic; TeachMePhysiology).
One-sentence takeaway: During sleep, awareness changes—especially in deep NREM—but the brain can still register some information and wake you if needed.
Callout: Sleep ≠ coma/anesthesia.

What Do We Mean by “Consciousness” During Sleep?
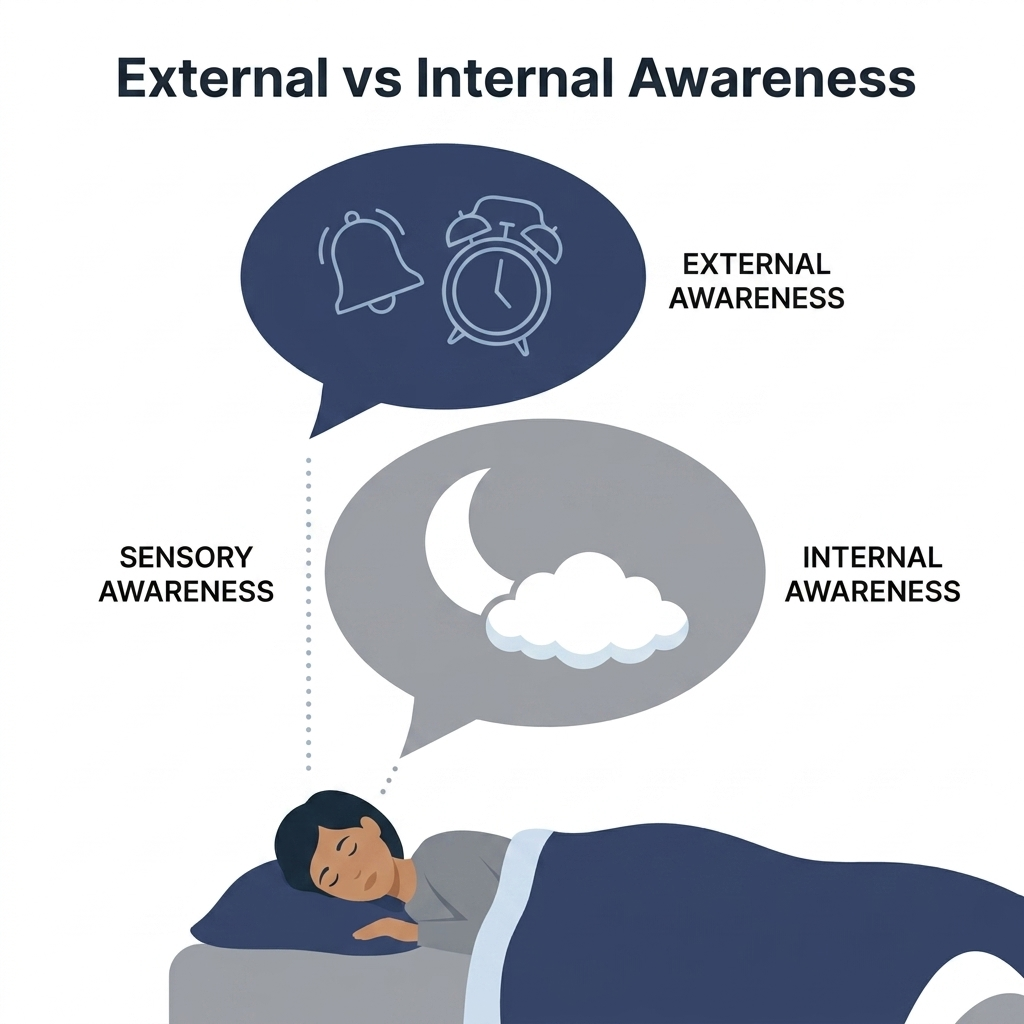
When people wonder “are you unconscious when you sleep?” they’re often talking about two kinds of awareness. External awareness: how much you can perceive and respond to the world—sounds, touch, your name, an alarm. Internal awareness: your mind’s experience while asleep—dreams, emotions, imagery, and memory fragments.
Both can exist in sleep, but they vary by stage. You might be hard to wake (low external awareness) while still having an intense dream (high internal awareness) (TeachMePhysiology; NCBI Bookshelf).
A helpful analogy: a dimmer switch, not an on/off button. As you move into deeper stages, responsiveness to the outside world turns down—not off.
Why you can still wake up: The brainstem and autonomic nervous system regulate vital functions during sleep. The sleeping brain stays more responsive to salient or threatening cues (smoke alarm, a baby crying, urgent discomfort), even if you don’t recall those signals later (NCBI Bookshelf; Cleveland Clinic). In short: sleep reduces responsiveness, but it does not sever awareness entirely.
The Stages of Sleep—and How Awareness Changes in Each
Across the night, most adults cycle repeatedly through NREM sleep (N1, N2, N3) and REM sleep, with cycles often averaging around 90 minutes (varies by person and night) (NCBI Bookshelf; Cleveland Clinic). Each stage has its own blend of external responsiveness and internal experience.
N1 (light sleep): Transition from wakefulness to sleep. Easy to wake; thoughts may drift; hypnic jerks are common. If awakened, many people say they “weren’t asleep” because awareness still feels partly online (Cleveland Clinic; NCBI Bookshelf).
N2 (stable sleep): External awareness decreases further; less likely to respond to light noises; still easier to wake than from deep sleep. N2 often makes up a large share of total sleep time in adults (NCBI Bookshelf; Cleveland Clinic).
N3 (deep/slow-wave sleep): Minimal external responsiveness; hardest stage to wake from. If awakened, disorientation or intense grogginess (sleep inertia) is common. The brain remains active in a different mode with a higher threshold for waking (NCBI Bookshelf; TeachMePhysiology).
REM sleep: Vivid dreams and strong “internal consciousness,” with brain activity that in some ways resembles wakefulness and typical muscle atonia. External responsiveness stays reduced (Sleep Foundation; NCBI Bookshelf).
Bottom line: Stages shift your balance of external responsiveness and internal experience across the night.

Is Sleep the Same as Being Knocked Out (Anesthesia) or in a Coma?
Because sleep can look like “unconsciousness,” it’s natural to ask whether sleep is basically the same as a coma or sedation. It isn’t.
Sleep vs coma: Coma involves profound impairment of arousal and awareness and does not follow normal sleep-stage cycling. Natural sleep is generally reversible with appropriate stimulation, even from deep sleep (TeachMePhysiology).
Sleep vs anesthesia/sedation: Anesthesia is a medically induced loss of responsiveness that alters brain networks differently than natural sleep. Sleeping through an alarm usually reflects sleep stage timing, sleep debt, alcohol, sedatives, or a sleep disorder—not anesthesia-like unconsciousness (TeachMePhysiology; NCBI Bookshelf).
In short: Natural sleep is reversible and structured; coma and anesthesia are not typical sleep states.

Can Your Brain Hear You While You Sleep?
What kinds of sounds can still get through? Salient cues like your name or a baby crying, threatening or urgent sounds like alarms, and repeated stimuli that become harder to ignore. This is often called residual awareness—some processing occurs even if you don’t recall it later (NCBI Bookshelf).
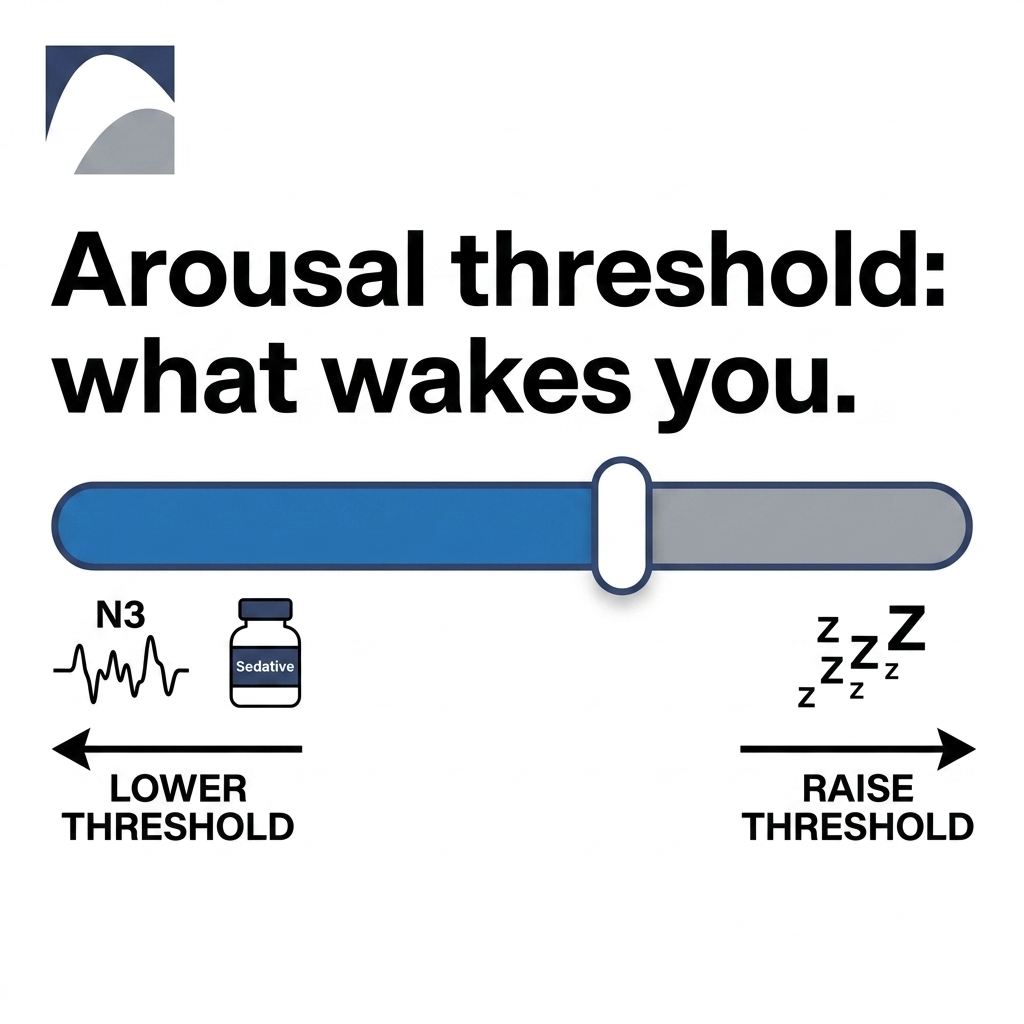
Why you sometimes don’t respond: Arousal threshold rises with deep NREM (N3), sleep deprivation, alcohol or sedating medications, and irregular sleep schedules. The brain may register a sound without fully waking you—especially in deep sleep. This also explains why two people can sleep through very different things in the same room (NCBI Bookshelf; Cleveland Clinic).
In short: The sleeping brain can pick up meaningful signals, but whether you wake depends on your arousal threshold.
Symptoms: Signs Your “Sleep Consciousness” Might Be Off
Most variations in sleep awareness are normal. Brief confusion when awakened from deep sleep, occasional vivid dreams or nightmares, and occasional sleep talking are common with stress, illness, travel, or schedule changes.
Signs to mention to a clinician include regular sleepwalking or complex behaviors during sleep, acting out dreams (especially with injuries), waking up gasping or choking or loud snoring with pauses, and severe daytime sleepiness, microsleeps, or concentration and memory problems.
To get a sense of daytime sleepiness, see the Epworth Sleepiness Scale. If you’re unsure where to start, review when to see an ENT for sleep problems.
In short: Occasional quirks are common, but safety risks, breathing symptoms, or severe sleepiness deserve evaluation.
Causes: What Influences How “Unconscious” You Feel During Sleep?
Normal factors that deepen sleep include prior sleep loss (sleep debt), heavy exercise or physical exertion, and individual differences across age and genetics.
Alcohol and sedatives can increase grogginess and reduce responsiveness, sometimes worsening sleep inertia or fragmenting sleep later in the night.
Sleep disorders can disrupt normal awareness and arousal. Examples include obstructive sleep apnea (which can fragment sleep and contribute to daytime “fog”), parasomnias (sleepwalking, confusional arousals), and REM-related disorders like REM sleep behavior disorder (NCBI Bookshelf; Sleep Foundation).
In short: Sleep depth and responsiveness vary with sleep debt, substances, and health conditions.
Treatments and What Helps
This section is educational—not a substitute for individualized care. Treatment choices depend on the cause and should be discussed with a qualified healthcare provider.
Sleep-hygiene basics that support healthy cycling: keep consistent sleep and wake times, get morning light exposure, reduce late-day caffeine, limit alcohol close to bedtime, and create a wind-down routine with fewer screens. See sleep hygiene tips (Cleveland Clinic).
If symptoms suggest sleep apnea or disrupted sleep, evaluation may include discussion of symptoms and, when appropriate, sleep testing (home or in-lab). Depending on the diagnosis, options may include CPAP, oral appliances, positional therapy, or addressing contributing nasal blockage when appropriate (Cleveland Clinic).
If unusual behaviors occur (sleepwalking, dream enactment), management commonly focuses on improving sleep regularity, reviewing alcohol and medication effects, making the sleep environment safer, and considering referrals when symptoms suggest specific disorders.
In short: Work with a clinician to match solutions to the specific cause.
Lifestyle Tips: How to Wake Up More Clearly
Use smart alarms that aim to time waking during lighter sleep windows when possible, and seek bright light soon after waking to encourage alertness.
Make mornings easier if you’re groggy: hydrate, do brief gentle movement, and avoid repeated snoozing if it worsens inertia.
Track patterns—bedtime, wake time, naps, alcohol intake, stress levels, and unusual nighttime events. If grogginess is severe, worsening, or persistent, consider medical evaluation.
In short: Gentle structure, light, and timing can ease morning inertia; seek care if grogginess is significant or ongoing.
FAQs About Sleep and Consciousness
Are you truly unconscious when you sleep? Not in the medical sense. Sleep is best described as altered consciousness: responsiveness drops (especially in deep NREM), but the brain remains active and can still process some information (TeachMePhysiology; NCBI Bookshelf).
Why can I wake up to some noises but not others? The brain prioritizes salient or threatening sounds, and your sleep stage matters. Deep NREM raises arousal threshold; sleep deprivation and alcohol can raise it further (NCBI Bookshelf).
Is REM sleep “lighter” than deep sleep? Deep NREM (N3) generally has the lowest external responsiveness. REM often features vivid dreams and strong internal experience, while external responsiveness remains reduced (Sleep Foundation).
Is sleep like a coma? No. Normal sleep cycles through predictable stages and is typically reversible with stimulation, unlike coma (TeachMePhysiology).
Can you learn or absorb information while asleep? The sleeping brain can process some simple or meaningful stimuli, but complex learning during sleep is limited (NCBI Bookshelf).
When should I see a doctor about sleep behaviors or extreme grogginess? Consider evaluation if symptoms involve safety risks, significant breathing symptoms, or severe daytime sleepiness affecting daily life.
In short: Sleep is not empty unconsciousness; it’s a dynamic state with variable awareness.
When to Get Help
If your concerns go beyond occasional grogginess—especially if you notice loud snoring with choking or gasping, extreme daytime sleepiness, or risky nighttime behaviors—an evaluation can clarify what’s going on and what options may improve sleep quality.
To learn more about next steps, visit Sleep and Sinus Centers of Georgia, explore when to see an ENT for sleep problems, and book an appointment if you’d like personalized help understanding symptoms and testing options.
In short: If symptoms raise safety or health concerns, getting evaluated is a smart next step.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.