

Adenoidectomy vs Tonsillectomy for Children: Which Surgery Does Your Child Need?
Parents often hear “tonsils” and “adenoids” discussed together—especially when a child snores, gets frequent infections, or struggles with chronic congestion or ear fluid. But these are two different tissues, and the “right” procedure depends on why symptoms are happening.
Think of the tonsils and adenoids as immune system “speed bumps” in the airway—they help the body recognize germs, but when they’re chronically inflamed or simply too large for a child’s airway, they can become part of the problem. That’s why ENTs focus less on the name of the surgery and more on the goal: fewer documented infections, better sleep breathing, clearer nasal airflow, or fewer ear-fluid problems.
This guide explains the key differences, the most common reasons surgeons recommend each procedure, what research and guidelines say, and what recovery typically looks like—so you can feel prepared for an ENT visit at Sleep and Sinus Centers of Georgia.
Quick Answer: What’s the Difference Between Tonsillectomy and Adenoidectomy?
Tonsils vs adenoids (simple anatomy)
- Tonsils sit at the back of the throat and are usually visible when your child opens their mouth wide.
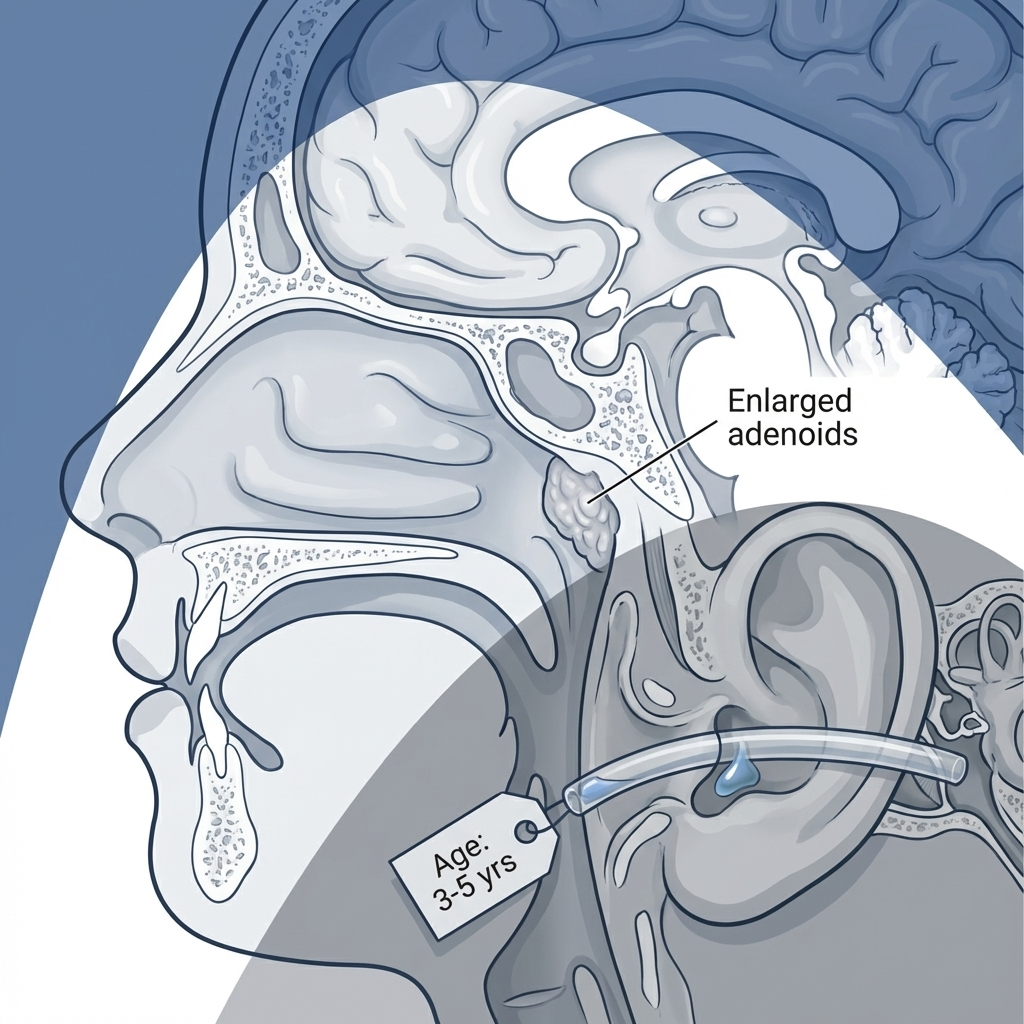
- Adenoids sit higher up behind the nose (where the back of the nose meets the throat). You typically can’t see them by looking in the mouth.
A simple way to picture it: tonsils are “at the doorway” of the throat, while adenoids are “upstairs behind the nose.” Both can affect breathing, but they tend to cause different day-to-day symptoms.
If you want a simple symptom-based comparison, see our post on big adenoids vs big tonsils: signs, key differences, and symptoms explained: https://sleepandsinuscenters.com/blog/big-adenoids-vs-big-tonsils-signs-key-differences-and-symptoms-explained
Why doctors sometimes remove one, the other, or both
In general:
- Tonsillectomy (removing tonsils) is most often considered for:
- recurrent, well-documented throat infections, or
- sleep-disordered breathing when tonsils contribute to blockage [1].
- Adenoidectomy (removing adenoids) is most often considered for:
- nasal blockage/mouth-breathing, chronic “stuffy nose,” or chronic adenoiditis [4], and sometimes
- persistent middle-ear fluid (otitis media with effusion, OME) in select situations—often in older children and/or when paired with ear tubes [3].
Many sleep-breathing cases are treated with adenotonsillectomy (both tonsils and adenoids removed) when appropriate, but decisions are individualized after ENT evaluation [1, 4].
Summary: In short, tonsillectomy targets throat infections and throat-level blockage, while adenoidectomy targets nose-level blockage and, selectively, chronic ear fluid.

Common Symptoms That Lead Parents to Ask About Surgery

Throat-focused symptoms (often point toward tonsils)
Parents commonly ask about adenoidectomy vs tonsillectomy for children when a child has:
- frequent sore throats
- fever with throat illnesses
- swollen neck glands
- repeated missed school or repeated antibiotic courses
A practical example: a parent might say, “It feels like we’re at urgent care every few weeks for strep,” or “We’ve had multiple antibiotic prescriptions this year.” Those details help the ENT determine whether episodes meet guideline-based thresholds.
Sleep and breathing symptoms (tonsils and/or adenoids)
Sleep symptoms are a major driver of evaluation:
- loud snoring most nights
- pauses in breathing, choking/gasping, or restless sleep
- morning headaches, daytime sleepiness, or behavioral concerns that seem tied to poor sleep
These symptoms can be part of sleep-disordered breathing in kids and may raise concern for obstructive sleep apnea in children [1].
A common pattern families describe is loud snoring, tossing/turning, and a child who wakes up cranky or seems unusually tired—even after “a full night” in bed.
Nose-focused symptoms (often point toward adenoids)
Adenoids are frequently involved when there’s:
- chronic nasal congestion (especially without obvious colds)
- chronic mouth-breathing
- “nasal” or muffled speech
- chronic runny nose
You can also read about mouth breathing and sleep quality and why it matters: https://sleepandsinuscenters.com/blog/chronic-mouth-breathing-and-its-impact-on-sleep-quality-causes-and-solutions-cdd3c
One simple clue: if your child’s nose seems “blocked” most days without an active cold—and it’s been going on for months—that’s a common reason ENTs take a close look at the adenoids.
Ear-focused symptoms (may involve adenoids + ear tubes)
Adenoids can contribute to ear issues because they sit near the opening of the Eustachian tubes. Families may notice:
- persistent middle-ear fluid (otitis media with effusion, OME)
- frequent ear infections
- hearing concerns or speech/language impact
Related: chronic ear fluid (OME) and hearing loss: https://sleepandsinuscenters.com/blog/chronic-ear-fluid-and-hearing-loss-causes-symptoms-treatment
A common example is a child who keeps “turning the volume up,” asks “What?” often, or has repeated reports of “fluid behind the eardrum” at pediatric visits.
Summary: The symptoms that matter most are where the problem shows up—throat, sleep, nose, or ears—because that guides which surgery (if any) might help.
What Causes Enlarged Tonsils or Adenoids in Children?
Normal immune tissue growth in childhood
Tonsils and adenoids are part of the immune system. In many children, they’re naturally larger in early childhood and may shrink later. Many children may experience improvement or outgrow certain symptoms over time; however, not all will, and ongoing monitoring is important.
Recurrent or chronic infections
Repeated viral and bacterial illnesses can inflame these tissues. Some children develop chronic inflammation (for example, chronic adenoiditis). Swollen tissue can narrow the airway, congestion can worsen, sleep quality can drop, and recovery from the next illness can be harder.
Allergies or chronic nasal inflammation
Ongoing nasal irritation—often seasonal or environmental—can contribute to swelling and congestion. Even when allergies play a role, removal isn’t automatically needed; the decision is usually symptom-based. Treating allergies can reduce “background inflammation,” but it won’t always fix a physical blockage if adenoids are significantly enlarged.
Anatomy + airway size (why some kids obstruct more easily during sleep)
Even “moderate” tissue size can matter if a child’s airway is relatively narrow. During sleep, muscle tone relaxes, which can make obstruction more noticeable. Parents sometimes notice this mismatch: “They breathe okay during the day, but nights are rough.” That difference is a classic feature of pediatric sleep-disordered breathing.
Summary: Enlarged tonsils or adenoids often reflect a mix of growth, infections, inflammation, and airway size—so the best plan depends on the child’s overall pattern.
When Tonsillectomy Is Usually Recommended (and When It’s Not)
Tonsillectomy for recurrent throat infections (Paradise criteria)
Guidelines support tonsillectomy for recurrent infections only when strict frequency and documentation criteria are met—often referred to as the Paradise criteria [1]:
- 7 or more episodes in 1 year, or
- 5 or more episodes per year for 2 years, or
- 3 or more episodes per year for 3 years
A key point: episodes should be documented in the medical record (not just remembered). What “counts” can vary, but documentation of findings like fever, swollen glands, tonsillar exudate, or positive strep testing is often important [1].
For a deeper dive, see recurrent strep throat vs tonsillectomy: when surgery is necessary: https://sleepandsinuscenters.com/blog/recurrent-strep-throat-vs-tonsillectomy-when-surgery-is-necessary

Expected benefit for infections (set realistic expectations)
Even for children who meet criteria, research suggests the benefit can be modest, often most noticeable in the first year after surgery for many children [2]. Clinicians often describe the goal as fewer severe, documented episodes rather than complete elimination of sore throats. While benefits are often modest, surgery carries risks which families should discuss with their surgeon.
When watchful waiting is preferred
If infections do not meet Paradise criteria, guidelines commonly recommend watchful waiting, because many children improve over time and the surgical advantage may be limited [1, 2]. For some families, watchful waiting is also a strategy with a purpose: carefully tracking future episodes so the next decision is clearer and evidence-based.
Summary: Consider tonsillectomy for well-documented, frequent infections or for sleep-related obstruction—otherwise, watchful waiting is often appropriate.
When Adenoidectomy Is Usually Recommended (and When It’s Not)
Adenoidectomy for nasal obstruction
Adenoidectomy in children is commonly considered when enlarged or chronically inflamed adenoids are contributing to:
- chronic mouth-breathing
- persistent nasal blockage
- sleep disruption tied to nasal obstruction [4]
A parent might notice: “They always sleep with their mouth open,” or “They sound congested even when they aren’t sick.” When adenoids are the main driver, removing them can improve nasal breathing and reduce the “stuffy all the time” feeling [4].
Adenoidectomy for chronic adenoiditis
If a child has persistent nasal drainage and recurrent symptoms despite appropriate medical treatment, adenoidectomy may be considered [4]. In practical terms: if your child keeps cycling through congestion and drainage without a clear break—even with reasonable medical care—your ENT may consider whether the adenoids are acting like a chronically inflamed reservoir.
Adenoidectomy for persistent middle-ear fluid (OME) in select kids
For otitis media with effusion (persistent middle-ear fluid), adenoidectomy may be considered in select situations—often in children over 4 years and/or as an adjunct to ear tubes, depending on the overall picture [3]. Evidence suggests it may modestly reduce persistence of OME, but improvements in hearing and quality of life remain uncertain based on current evidence [3]. Here, “uncertain” means research results are mixed or insufficient to show a consistent benefit across children.
Summary: Consider adenoidectomy for chronic nasal blockage or adenoiditis—and selectively for persistent ear fluid in older children—after discussing likely benefits and limits.
When Children Need Both Removed (Adenotonsillectomy)
Obstructive sleep-disordered breathing / suspected pediatric OSA
One of the most common reasons families compare adenoidectomy vs tonsillectomy for children is snoring and sleep issues. For obstruction-related sleep symptoms, guidelines commonly support tonsillectomy—often with adenoidectomy—when these tissues are contributing to blockage [1]. When the history and exam support obstruction, removing both tissues can address blockage at more than one level of the airway [1, 4]. Importantly, this is not “one size fits all”—your ENT will individualize recommendations.

When a sleep study (polysomnography) is recommended first
A sleep study may be recommended before surgery for certain children, especially:
- children under 2 years, or
- children with specific risk factors or comorbidities (your clinician will review these based on history and exam) [1]
A sleep study can act like a “map” of breathing during sleep—helpful when the risk profile is higher or when symptoms and exam do not line up neatly.
Summary: When sleep obstruction is the main problem, adenotonsillectomy is often considered—guided by your child’s history, exam, and in some cases a sleep study.
How ENTs Decide: Evaluation and Tests You Might Expect
History + documentation
You may be asked about:
- how many infections occurred (and when)
- fever history, strep testing results, and antibiotics used
- missed school and symptom pattern over time
Tip: bringing a simple timeline (dates of sore throats, urgent care visits, strep tests, antibiotic names) can make the visit more efficient and the recommendation more confident.
Physical exam
- Tonsil size can be evaluated directly.
- Adenoids are often assessed indirectly based on symptoms and nasal exam.
Nasal endoscopy or imaging (when needed)
Sometimes a small camera exam helps evaluate adenoid size and nasal anatomy, especially when symptoms don’t match what’s seen on a routine exam.
Hearing testing / tympanometry (for ear fluid concerns)
If OME or hearing concerns are part of the story, hearing tests and tympanometry can add useful information.
Sleep evaluation
Clinicians may use screening questions and, for appropriate children, consider polysomnography [1].
Summary: The best recommendations come from a clear history, focused exam, and targeted testing when the picture isn’t straightforward.
Benefits vs Limits of Each Surgery (What Research Shows)
Tonsillectomy benefits
- Infections: modest short-term reduction in sore-throat episodes in many children who meet criteria [2].
- Sleep-disordered breathing: often improves sleep symptoms and sleep quality when enlarged tonsils/adenoids contribute to obstruction [1].
Adenoidectomy benefits
- Nasal obstruction: often improves nasal breathing when adenoids are a main contributor [4].
- OME: may reduce persistence in select older children, but hearing and quality-of-life improvements remain uncertain in the evidence [3].
What surgery cannot guarantee
No procedure guarantees:
- zero colds or sore throats
- a cure for allergies
- that all snoring will disappear (not all snoring is obstructive sleep apnea)
This is why discussions about adenoidectomy vs tonsillectomy for children usually focus on specific goals (sleep quality, infection frequency, nasal airflow, ear fluid patterns).
Summary: Surgery can help the right problems in the right child—but setting realistic, goal-based expectations is essential.
Risks and Side Effects Parents Should Know (Both Surgeries)
Common short-term issues
- pain (generally more significant after tonsillectomy)
- temporary bad breath
- reduced appetite or disrupted sleep for a period of time [1]
Families can expect a “recovery rhythm”: a few tougher days, then gradual improvement—while staying alert for red flags your surgical team reviews.
Dehydration risk
Pain can reduce drinking, which increases dehydration risk. Planning pain control and hydration strategies with your surgical team matters.
Bleeding risk
Post-operative bleeding is a known risk after tonsil surgery and can require urgent evaluation. Your ENT team will review what to watch for and when to seek urgent care [1].
Anesthesia risks
Anesthesia is generally safe, but risk varies based on a child’s health profile and any airway/sleep issues—another reason pre-op evaluation is important [1].
Summary: Every surgery has risks; understanding pain control, hydration, and bleeding plans helps keep recovery on track.
Recovery Timeline and Home Care Tips (Practical, Parent-Focused)
Tonsillectomy recovery (typical expectations)
Many children have:
- sore throat for 7–10 days (sometimes longer)
- referred ear pain (ear pain that “comes from” the throat)
- variable energy and sleep for about 1–2 weeks
Setting expectations with siblings and school can help: recovery is real, and it’s normal if your child isn’t “back to 100%” immediately.
Adenoidectomy recovery (typical expectations)
Adenoidectomy alone is often easier:
- mild sore throat
- nasal congestion or temporary snoring that can briefly worsen before improving
A child may sound stuffier for a short period, then breathe more clearly as swelling settles.
Eating and drinking tips to prevent dehydration
Families are often encouraged to prioritize fluids and choose easy-to-swallow foods during early recovery. Your surgical team will provide specific instructions.
Activity restrictions and return to school
Return-to-school timing and activity limits vary by procedure and child; many families plan for time at home and a gradual return to normal routines.
Warning signs after surgery (when to call the doctor or go to ER)
Your post-op instructions may highlight urgent concerns such as:
- bleeding
- trouble breathing
- signs of dehydration (very low urine output, lethargy, inability to keep fluids down)
- pain not controlled with the plan provided by your clinician [1]
Summary: Expect about a week of throat pain after tonsillectomy and a shorter course after adenoidectomy—focus on pain control, fluids, and clear red-flag plans.
Alternatives and “Try This First” Options (When Appropriate)
For recurrent infections not meeting Paradise criteria
Guidelines often favor watchful waiting, plus careful documentation of future episodes [1, 2]. A useful next step is to keep a running list of throat infections, where they were treated, and what testing was done.
For nasal obstruction
Depending on the cause, options may include allergy evaluation/management, nasal saline, and clinician-directed medications.
For ear fluid
OME may be observed, treated with ear tubes, or considered for tubes plus adenoidectomy in age- and situation-dependent ways—keeping in mind hearing and quality-of-life benefits are uncertain in some evidence summaries [3].
Summary: When surgery isn’t clearly indicated, structured observation and targeted medical therapy can be valuable first steps.
Shared Decision-Making: Questions to Ask Your ENT
If the recommendation is tonsillectomy
- “Do we meet Paradise criteria based on documented infections?” [1]
- “What benefit should we realistically expect—and for how long?” [2]
If the recommendation is adenoidectomy
- “Is this mainly for nasal obstruction, chronic adenoiditis, or ear fluid?” [4]
- “If this is for OME, what do we know about hearing improvement in my child’s situation?” [3]
If sleep-disordered breathing is the concern
- “Do we need a sleep study first?” [1]
Safety planning
- “What’s our bleeding plan, pain-control plan, and hydration plan?”
Summary: Clear questions—and good documentation—make it easier to match treatment to your child’s goals and risks.
FAQs
Can my child have an adenoidectomy without removing tonsils?
Yes. When symptoms are mainly nasal (chronic congestion/mouth-breathing) or certain ear-fluid patterns, adenoidectomy alone may be considered [4].
Does tonsil size alone mean my child needs surgery?
Not necessarily. Decisions usually depend on symptoms (sleep, infections, quality of life) and guideline-based criteria—not size alone [1].
Will removing adenoids help my child’s hearing?
In children with OME, adenoidectomy may reduce persistence of fluid in select cases, but research finds hearing and quality-of-life improvement is uncertain overall [3].
Is tonsillectomy “worth it” for frequent sore throats?
It depends on whether infections meet Paradise criteria and are well documented. When criteria aren’t met, watchful waiting is often preferred; when they are met, the average benefit is often modest and most noticeable over about a year for many children [1, 2].
Will surgery cure my child’s snoring?
If snoring is due to airway obstruction from tonsils/adenoids, surgery often helps. But not all snoring is obstructive sleep apnea, and some children may need a sleep study first [1].
What age is best for these surgeries?
There isn’t one “best” age. Evaluation is individualized, and guidelines recommend extra consideration (including possible sleep study) for very young or higher-risk children with sleep-related concerns [1].
What are the most important post-op red flags?
Bleeding, breathing difficulty, and signs of dehydration are commonly emphasized as urgent concerns in post-op planning [1].
Conclusion: Choosing the Right Surgery (or Choosing to Wait)
When comparing adenoidectomy vs tonsillectomy for children, the most evidence-supported reasons tend to be:
- Tonsillectomy: best supported for Paradise-criteria recurrent infections and obstructive sleep-disordered breathing [1, 2].
- Adenoidectomy: best supported for nasal obstruction/chronic adenoiditis, and selectively for persistent OME in older children, with uncertain hearing impact [3, 4].
Because these procedures involve real tradeoffs (pain, bleeding risk, dehydration risk, anesthesia considerations), shared decision-making and careful selection matter.
If your child has ongoing sleep-breathing symptoms, recurrent documented infections, or persistent nasal/ear concerns, you can book an appointment with Sleep and Sinus Centers of Georgia at https://www.sleepandsinuscenters.com/ to review options.
Summary: The “right” choice is the one that matches your child’s symptoms, evidence-based indications, and your family’s goals after a thoughtful discussion with your ENT.
References
1. AAO-HNSF Clinical Practice Guideline: Tonsillectomy in Children (2019). https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/aao-guidelines-tonsillectomy-2019.pdf
2. Cochrane Review (2014): Tonsillectomy or adenotonsillectomy vs non-surgical treatment. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001802.pub3/information
3. Cochrane Review (2023): Adenoidectomy for otitis media with effusion (OME). https://pmc.ncbi.nlm.nih.gov/articles/PMC10591285/
4. AAO-HNS Clinical Indicators: Adenoidectomy (2022). https://www.entnet.org/resource/clinical-indicators-adenoidectomy/
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Don’t let allergies slow you down. Schedule a comprehensive ENT and allergy evaluation at Sleep and Sinus Centers of Georgia. We’re here to find your triggers and guide you toward lasting relief.






